Erectile dysfunction has been a taboo topic in Asian countries, but related research has been increasing recently. The reported prevalence of ED in Asian countries varies greatly, from 2% to 88%.1 A recent meta-analysis summarized age-specific prevalence rates as follows: 15% for ages 20 to 29, 30% for 30 to 39, 41% for 40 to 49, 54% for 50 to 59, and 70% for 60 to 69.2 The rate is even higher among men with chronic diseases including diabetes, according to an international study including two Asian countries.3 The prevalence of ED among men with diabetes also varies widely, from 35% to 90%.4 The risk of developing ED is about 3 times higher in diabetic men compared to those who do not have diabetes.5,6 Most of the data on ED in diabetics are from non-Asian countries. In a few studies conducted in Vietnam, the frequency of ED was found to be 40% in the general population over 40 years of age, and 65.3% in those with type 2 diabetes.7,8 While these locally published studies reflect an increasing awareness of ED in the country, practical recommendations for diabetes specialists are limited.
In this study, the International Index for Erectile Function Questionnaire (IIEF-5), an internationally accepted and practical measure, was used to estimate the prevalence of ED and investigate its associated factors among Vietnamese men with diabetes visiting a general public hospital in Ho Chi Minh City. The aim was to present recommendations for Vietnamese diabetes specialists that can be easily applied in their clinical practice.
We conducted a cross-sectional investigation between August 2011 and March 2012 at the People’s Hospital 115 in Ho Chi Minh City, Vietnam. Formerly a military clinic, it is now a tertiary university-affiliated general hospital with 1500 beds. On the average, the hospital receives about 100 outpatients with diabetes per day. The subjects were recruited by convenience sampling from an outpatient clinic. Criteria for inclusion were male gender, diagnosed with type 2 diabetes, age 30 to 65 years and currently married. Exclusion criteria were concomitant chronic diseases such as kidney, liver or chronic obstructive pulmonary disease; and the inability to complete a self-administered questionnaire due to eye or extremity disabilities.
During the study period, the affiliated physician-researchers recruited 151 patients that they encountered for a total of 34 days. Survey days were selected according to the researchers’ schedule. Efforts were made to ensure patient privacy while accomplishing the questionnaires. Male physicians were in attendance.
We used IIEF-5 to assess erectile dysfunction. Extracted from the original 15-item IIEF, this 5-item measurement is standardized and now widely used for the diagnosis and classification of ED severity.9 The 5 items assess erection confidence, erection firmness, maintenance frequency, maintenance ability and intercourse satisfaction in the past 6 months. The total score was the basis for classification of ED: no dysfunction (22-25), mild dysfunction (17-21), mild to moderate dysfunction (12-16), moderate dysfunction (8-11) and severe dysfunction (5-7). Since a Vietnamese language version was not available, we went through a rigorous back-translation procedure to ensure an accurate and culturally adequate translation. Initially, 3 Vietnamese native speakers independently translated the original English IIEF-5 into Vietnamese, then collectively discussed how to develop the first consensus version. Secondly, 2 English native speakers back-translated the first version into English. In the third step, we compared the original and back-translated English versions to finalize the Vietnamese language version. For the fourth step, we conducted a test-retest face-to-face survey among 20 volunteer diabetic patients with an interval of 4 weeks to examine reliability. Twenty-five patients were included in the first interview, but only 20 patients returned for the second. Spearman’s correlation coefficient of the two scores was 0.56; the mean difference in score was 0.4, with a standard deviation of 4.8. In addition, we paid careful attention to the order and layout of questions to make the questionnaire easy to fill out by Vietnamese patients.
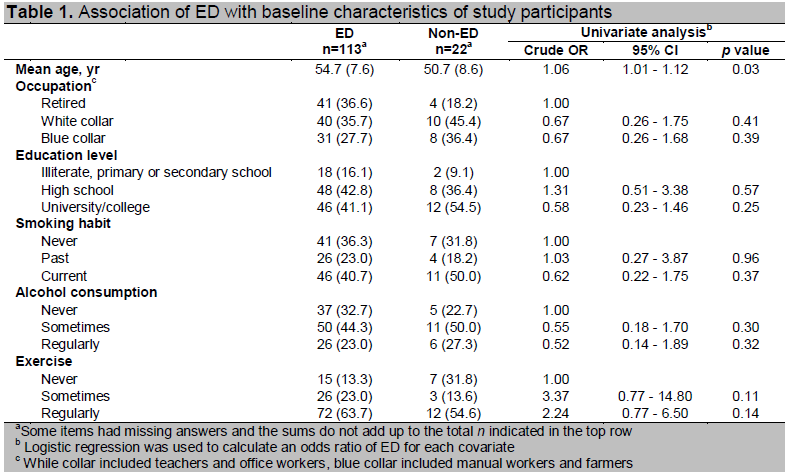
Other survey items included age, socioeconomic status (occupation and education level), lifestyle (smoking, alcohol consumption, physical activity), diabetes treatment history, family history of diabetes, medical history (stroke, cardiovascular disease and foot ulcer), and mental state as measured by the WHO-Five Well-being Index.10 Anthropometrics included height (m), weight (kg) and waist circumference (cm).
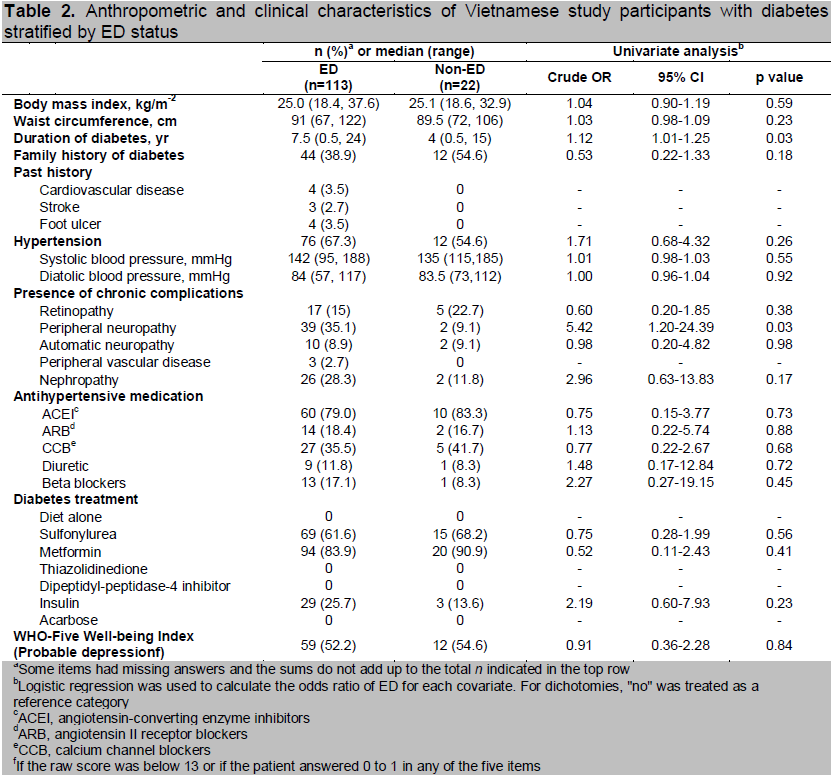
Patients were diagnosed with diabetic peripheral neuropathy if they showed at least one abnormal result in any of 3 tests: superficial pain testing, light touch perception and vibration sensation using a 128-Hz tuning fork. For sensory testing, the patient was required to close his eyes and was given a sample test on the forearm. The patient was then asked about the characteristics of the sensation. He was then asked to identify the sensation experienced upon application of the test at the dorsum of the first toe, and the plantar aspect of the distal phalanx of the first, third, and fifth toe of each foot. The test was defined abnormal when no sensation was elicited.11 For vibratory testing, a 128-Hz tuning fork was placed on the bony prominences at the dorsum of the big toe. The patient was asked to say when he began to sense a decrease in vibration. The tuning fork was then moved to the dorsal aspect of the distal phalanx of the examiner’s thumb. The time (s) was estimated when vibration sensation diminished beyond the examiner’s perception. The abnormal value was between 0 and 10 seconds.12
The presence of retinopathy was detected by fundus examination. Peripheral vascular disease was assessed by palpation of the dorsalis pedis pulse and/or Doppler ultrasonography. Autonomic neuropathy was evaluated by taking the patient’s pulse rate at rest (more than 100 beats per minute) and/or orthostatic blood pressure gradient (more than 20 mmHg).
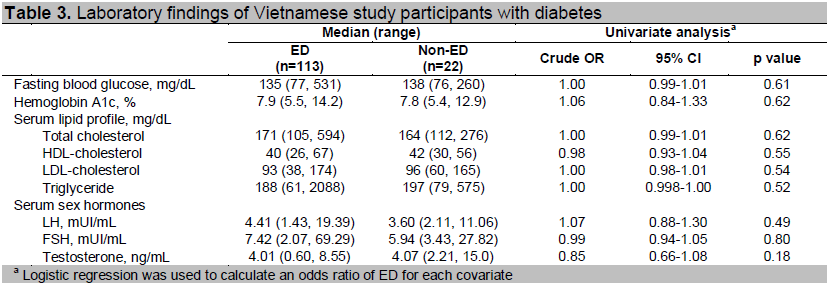
Blood samples were drawn and analyzed for fasting blood glucose, hemoglobin A1c (HbA1c), triglycerides, low-density lipoprotein (LDL) cholesterol, high-density lipoprotein (HDL) cholesterol, total cholesterol, testosterone, follicle-stimulating hormone (FSH) and luteinizing hormone (LH). Urine analysis including microalbuminuria was also performed.
Data were analyzed by Stata software version 12.0. Statistical significance was considered at p <0.05. Odds ratios of ED defined as an IIEF-5 score of 21 or lower for each survey item were calculated using logistic regression model. The first analyses estimated crude OR for each item listed in Tables 1 to 3, with ED as a dependent variable. The second multivariate analysis included significant factors in the first analyses because of potential confounding effects.
The study protocol was reviewed and approved by the Scientific Research Committee of People’s Hospital 115. All participants gave oral informed consent. Considering cultural adequacy, agreeing to and filling out a questionnaire was considered as giving consent to the survey.
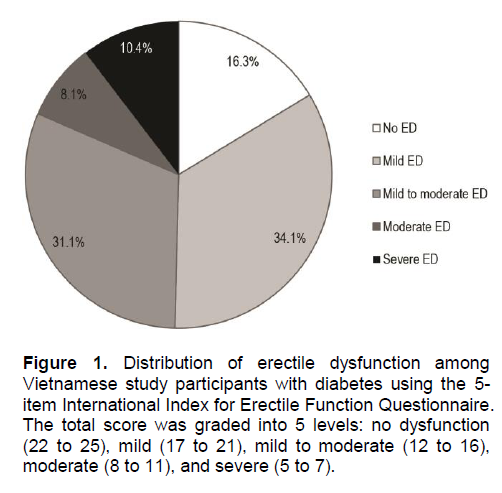
Of 151 patients invited, 135 completed the questionnaire, yielding a response rate of 89%. The responders and the 16 non-responders did not differ in age and duration of diabetes. The mean age of the responders was 54 years (SD 7.9), while the median duration of diabetes was 7 years (range 5 to 24). Twenty-four percent were treated with insulin, and median HbA1c was 7.9% (range 5.4 to 14.2). Using the IIEF-5, the overall prevalence of ED was 83.7%, of which 34.1% were mild, 31.1% mild to moderate, 8.1% moderate, and 10.4% severe (Figure 1).
Click here to download Figure 1
Figure 1. Distribution of erectile dysfunction among Vietnamese study participants with diabetes using the 5-item International Index for Erectile Function Questionnaire. The total score was graded into 5 levels: no dysfunction (22 to 25), mild (17 to 21), mild to moderate (12 to 16), moderate (8 to 11), and severe (5 to 7).
The risk for erectile dysfunction increased significantly with age (OR 1.06, 95%CI 1.01-1.12) and duration of diabetes (OR 1.12, 95%CI 1.01-1.25) (Tables 1 and 2). Similarly, the presence of diabetic peripheral neuropathy was found to be significantly associated with erectile dysfunction (OR 5.42, 95%CI 1.20-24.39) (Table 2). None of the laboratory findings showed significant association (Table 3).
Our study found that the prevalence of ED in men with diabetes was 83.7%. The percentage of men with diabetes-associated ED varies among studies due to age, duration of diabetes, study setting and measures used.4 Even with the same measurement, different cut-off values are suggested in different countries: an IIEF-5 score of 17 is applied in Korea, whereas 21 is applied in Italy.13,14 The prevalence of over 80% obtained in our study was in the upper end of the reported prevalence in Asian countries.2 A similar prevalence of 84.6% was reported among Chinese men with type 2 diabetes between 25 and 76 years of age.15
The observed high prevalence, despite cultural hesitation in the discussion of sexual issues in Vietnam, may be an overrepresentation caused by the selected study site, which was a tertiary referral hospital. Undetected ED cases, possibly from lack of physician awareness, may have left most ED cases untreated, and may have also increased its prevalence.
Age and duration of diabetes are important factors associated with ED as reported in previous studies and confirmed in our study.4,16-17 Disease duration was entered into a multivariate analysis with peripheral diabetic neuropathy and both remained significant. The association of peripheral diabetic neuropathy with ED has been reported in previous studies, including one from Japan by Sasaki and colleagues.18 The etiology of diabetic ED is multifactorial, with neuropathic, vasculopathic, hypogonadal and local pathologic changes.4,6 Diabetic neuropathy includes autonomic and peripheral neuropathy; the former impairs relaxation of the smooth muscle of the corpus cavernosum, and the latter impairs sensory conduction from the shaft and glans of the penis to the reflexogenic erectile center.4