Autoimmune disorders tend to coexist in the same subjects and there are well-known autoimmune overlap syndromes where systemic and organ-specific diseases are associated with each other.1-3 To date, a number of studies have demonstrated the association of autoimmune thyroid disease (ATD) with autoimmune rheumatic disorders (ARD).3-8 In the study by Biro et al,3 125 (8.2%) out of 1,517 systemic autoimmune patients had autoimmune thyroid disease, 5.7% with Hashimoto’s thyroiditis (HT) and 2.6% with Graves’ disease (GD). Mixed connective tissue disease (MCTD) and Sjögren’s Syndrome (SS) most frequently overlapped with autoimmune thyroid diseases (24 and 10%, respectively). The prevalences of HT and GD in systemic lupus erythematosus (SLE), rheumatoid arthritis (RA), systemic sclerosis (SSc), MCTD, SS, and polymyositis/dermatomyositis (PM/DM) were noted to be higher than that seen in the general population. Lazurova et al,4 found the prevalence of ATD at 24% among 80 patients with autoimmune rheumatic disorders (SLE or RA). Atzeni and colleagues9 noted an increased prevalence of anti-thyroid antibodies among RA patients but with a low prevalence of hormonal alterations. Of the 300 lupus patients in the retrospective analysis by Pyne and Isenberg,6 5.7% had hypothyroidism which is a higher prevalence than that for the normal background population (1%). Among 129 SLE patients in Singapore,10 8.5% had hyperthyroidism, 3.9% had Hashimoto’s thyroiditis, and 3.1% had subclinical hypothyroidism. In addition, the prevalence of Hashimoto’s thyroiditis was found to be 9.5% among Korean patients with SLE11 and 8.8% among Chinese SLE patients.12 The prevalence of Graves’ disease among Korean SLE patients was 4.8%. 11 In a review of medical records of 73 SLE patients at the University of Santo Tomas, anti-thyroid peroxidase antibody was present in 7% of the subjects.13
As a result of these observations, some authors2-4, 7 consider it clinically important to screen patients with systemic autoimmune diseases for the coexistence of thyroid disorders. Appenzeller and colleagues8 concluded in their study that since symptoms of SLE and thyroid disease can be similar, SLE patients should routinely be investigated for autoimmune thyroid disease. For RA, however, Goncalves et al14 do not recommend routine thyroid antibodies and thyrotropin tests in all patients.
Thyroid dysfunction meets many criteria for a condition justifying population screening because even mild derangements in thyroid function are associated with significant and reversible morbidities such as atrial fibrillation and reduced bone mineral density. This study aims to determine the local prevalence of autoimmune thyroid disease among patients with the different types of autoimmune rheumatic disorders, namely SLE, RA, SSc, MCTD, SS, and PM/DM. We used a clearly defined diagnostic work-up that includes thyroid function tests, thyroid autoantibodies and urinary iodide excretion. By checking thyroid autoantibodies, patients who truly have an autoimmune etiology for their thyroid dysfunction can be differentiated from those with steroid-induced derangements in thyroid function, as the majority of these patients will take it chronically to control of their rheumatic disorder. Urinary iodide excretion will also be determined to evaluate iodine deficiency as a probable cause of thyroid dysfunction.
A secondary aim of this study is to identify clinical features that may be associated with the occurrence of the disease to help clinicians identify autoimmune rheumatic patients who could probably have a concomitant autoimmune thyroid disorder. The data may later provide a basis for recommending guidelines for screening autoimmune thyroid disease in Filipino patients with these disorders. Identifying these patients and providing treatment for their thyroid dysfunction will help prevent the complications associated with these diseases adding to the morbidity of the existing autoimmune rheumatic disorder.
This is a cross sectional analytical study that included adult Filipinos (age 19 years and above) diagnosed with autoimmune rheumatic disorder(s) at the Philippine General Hospital. Sample size computed was 116 at 95% confidence level, 10% relative error, and assumed prevalence of autoimmune thyroid disease at 8.2% as seen in the study by Biro et al.3 Computation of the sample size was made through Epi Info 6.
All adult patients seen at the General Medicine, Family Medicine, and Rheumatology Clinics, as well as patients seen at the Emergency Room and those admitted at the Medical Wards, with a diagnosis of SLE, RA, SSc, MCTD, SS, or PM/DM based on diagnostic criteria16,17 and not known to have ATD were recruited from January to December 2011. Patients with features of limited cutaneous SSc coexisting with features of SLE, PM, and RA were classified as having MCTD. Written informed consent was obtained from all patients. The study was approved by the Clinical Research Division and the Expanded Hospital Research Office of the Philippine General Hospital.
Clinical characteristics were taken and recorded for each patient. Age, sex, presenting manifestation for the ARD, presence of goiter, smoking history, family history of thyroid disease, age at onset of the ARD, disease duration, current medications and presence of other illnesses were obtained. The physical examination for goiter was done by palpation by a single investigator. Serum thyrotropin (TSH), thyroxine (FT4), triiodothyronine (FT3), anti-thyroid peroxidase antibody (anti-TPO), anti-thyroglobulin antibody (anti-Tg), and urinary iodide excretion (UIE) were determined. The patients were classified into the different categories of thyroid autoimmunity (anti-TPO or anti-Tg positive or both) and thyroid dysfunction (subclinical and clinical hypothyroidism, subclinical and clinical hyperthyroidism). All patients diagnosed with ATD were referred to the Thyroid Clinic of the Philippine General Hospital Outpatient Department for further management.
Serum TSH was measured by the immunoradiometric assay method while FT4, FT3, anti-TPO, and anti-Tg were measured using the radioimmunoassay method. Commercial kits manufactured by Izotop, Institute of Isotopes Company, Ltd., Budapest, Hungary (Serum TSH, anti-TPO, anti-Tg) and Immunotech, Beckman Coulter Company, Prague, Czech Republic (FT4, FT3) were used. Reference ranges used were as follows: TSH 0.3 – 3.8 mIU/ml, FT4 11 – 24 pmol/L, FT3 2.2 – 6.8 pmol/L, anti-TPO < 100.0 U/ml, and anti-Tg < 50.0 UL/ml.
Urinary iodide excretion was determined using ammonium persulfate digestion with spectrophotometric detection of the Sandell –Kolthoff reaction.
Data were described using means ± SD, frequencies, and percentages. The prevalence of autoimmune thyroid disease among patients with autoimmune rheumatic disorders was computed by dividing the number of events by the number of population examined. Associations between qualitative clinical factors and ATD were carried out using chi-square test or Fisher’s exact test. Independent t-test was used to determine association of the different quantitative variables with ATD. A p ≤ 0.05 was considered significant.
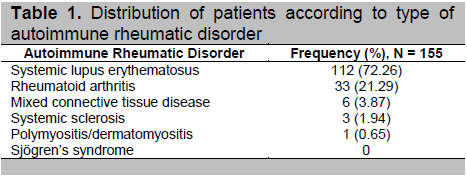
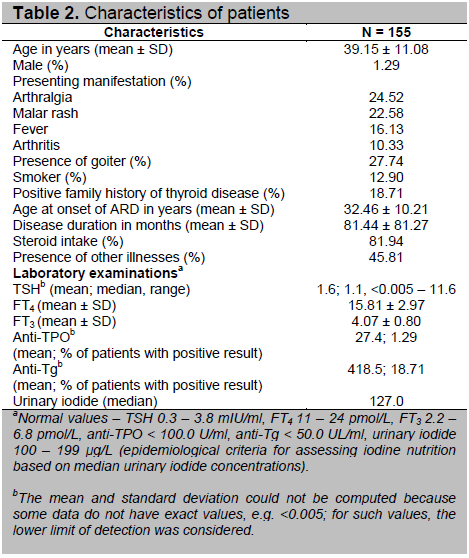
A total of 155 patients were included in the study. Three subjects previously known to have ATD were excluded. One hundred fifty three subjects (98.71%) were female and only 2 subjects were male. The mean age was 39±11.08 years old. Majority of the population was composed of patients with SLE followed by RA, MCTD, SSc, and PM/DM. None of the subjects had SS. The most common presenting manifestation was joint pain followed by malar rash, fever and arthritis. Other presenting symptoms such as alopecia, rash, body weakness, leg weakness, pedal edema, anasarca, photosensitivity, oral ulcer, muscle stiffness, nose bleeding, hematemesis, repeated abortion, anorexia, altered sensorium, easy fatigability, and dyspnea were noted in 1 – 6% of the population.
Forty three patients (27.74%) had goiter, 20 patients (12.90%) were either current or previous smokers, and 29 patients (18.71%) had family history of thyroid disease. The mean age at onset of ARD was 32 years old while mean duration of ARD was 81.44 months. One hundred twenty seven (81.94%) of the subjects were on steroids such as prednisone, methylprednisolone, dexamethasone, or hydrocortisone. Seventy one (45.81%) of them had other illnesses like hypertension, dyslipidemia, and diabetes. The mean anti-Tg level was above the normal value while the mean levels of TSH, FT4, FT3, and anti-TPO were within normal. The median UIE corresponded to adequate iodine intake. Characteristics of the patients are summarized in Table 2.
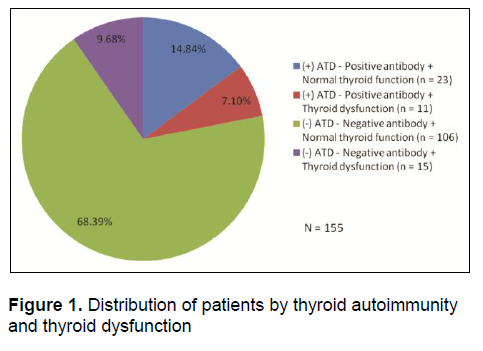
Thirty four of the 155 patients (21.94%) were noted to have autoimmune thyroid disease. Figure 1 shows the distribution of patients by thyroid autoimmunity and thyroid dysfunction. Thirty four patients were positive for anti-TPO and/or anti-Tg with or without accompanying subclinical or clinical thyroid dysfunction. Thus, the prevalence of autoimmune thyroid disease in this population was computed at 21.94% (14.84% positive antibody with normal thyroid function and 7.10% positive antibody with thyroid dysfunction). Fifteen patients (9.68%) had negative antibody but with thyroid dysfunction. The rest of the population (68.39%) had negative antibody and normal thyroid function. Anti-Tg positivity was more common than anti-TPO. Twenty nine patients (18.71%) had positive anti-Tg antibody, 2 patients (1.29%) were positive for anti-TPO antibody, and 3 patients (1.94%) had both antibodies. Among the patients diagnosed with ATD, 23 (67.65%) presented with antibody positivity without derangement in thyroid function. Thyroid dysfunction was noted in 26 out the 155 patients (16.77%). Eleven of the 34 patients with ATD (32.35%) had thyroid dysfunction while 15 of the 121 patients without ATD (12.40%) had abnormal thyroid function test. Eleven of the 26 patients with thyroid dysfunction (42.31%) were positive for thyroid antibodies. The most common category of thyroid dysfunction was subclinical hypothyroidism, noted in 12 subjects or in 7.74% of the population – 5 out of the 34 subjects with ATD (14.71%) and 7 out of 121 subjects without ATD (5.79%).
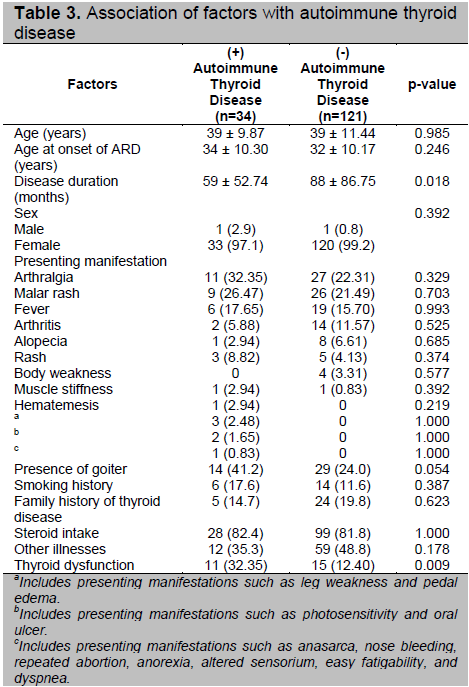
There was a significant association between duration of the autoimmune rheumatic disorder and autoimmune thyroid disease with a p= 0.018 (Table 4). A shorter duration of ARD (mean duration of 59 months compared to 88 months) was associated with ATD. No significant association was noted with the other clinical factors although there was an almost significant association observed for the presence of goiter (p-= 0.054). There was a significant association between thyroid dysfunction and ATD (p= 0.009). More patients with ATD have accompanying thyroid dysfunction compared to those without ATD (32.35% vs. 12.40%).
Click here to download Table 1
Table 1. Distribution of patients according to type of autoimmune rheumatic disorder
Click here to download Table2
Table 2. Characteristics of patients
Click here to download Figure 1
Figure 1. Distribution of patients by thyroid autoimmunity and thyroid dysfunction
The prevalence of autoimmune thyroid disease among Filipino patients with autoimmune rheumatic disorders in this study is 21.94%. This is in agreement with several observations that there was increased prevalence of ATD in this patient population. We actually found a higher prevalence compared to the study done by Biro et al3 who noted a prevalence of 8.2%. The association between systemic and organ-specific autoimmune diseases has been demonstrated in previous studies.3-5 At least one reason for this association is that both disorders share HLA-DR3 as a susceptibility factor. 2 Cross-reactivity of systemic autoantibodies with thyroid antigens or that of thyroid autoantibodies or autoreactive T cells with other tissues and organs may also explain the organ-specific and systemic (non-organ-specific) autoimmune disease overlaps. Cytokine imbalance may also account for the development of such overlaps. There may be two-way interactions between the pathogenic factors of thyroid and systemic autoimmunity leading to the perpetuation of both conditions.3 The study by Porkodi et al5 suggests a possible acceleration of autoimmune thyroiditis with the coexistence of SLE or RA.
Click here to download Table 3
Table 3. Association of factors with autoimmune thyroid disease
Among the patients diagnosed with ATD in this study, about two-thirds (23 out of 34) presented with anti-TPO and/or anti-Tg positivity without derangement in thyroid function while the remaining had positive thyroid antibodies with accompanying thyroid dysfunction. As stated by Pyne and Isenberg,6 both anti-Tg and anti-TPO have been found with greater frequency in SLE than in the general population, even in lupus patients who do not have clinical thyroid disease.
In the pathogenesis of endocrine autoimmunity, the production of organ-specific autoantibodies causes progressive immune-mediated destruction of endocrine tissues. Major organ destruction eventually causes secretory insufficiency and leads to clinical disease. This was demonstrated in the study by Appenzeller et al8 who noted that 71% of SLE patients who developed thyroid disease during follow-up presented previously with positive thyroid antibodies on more than one occasion.
In the Whickham survey,18 the odds ratios of developing hypothyroidism with positive anti-thyroid antibodies alone were 8 for women and 25 for men. In this study, the proportion of patients with thyroid dysfunction among those with positive antibodies was higher compared to those without thyroid antibodies (32.35% vs. 12.40%) and there was note of a significant association between thyroid dysfunction and ATD. Furthermore, 11 of the 26 patients with thyroid dysfunction (42.31%) were positive for thyroid antibodies.
As mentioned, thyroid dysfunction was noted in 26 patients – 11 patients with positive antibodies and 15 patients without antibodies. Possible causes of thyroid dysfunction in those with negative antibodies could be due to iodine deficiency or steroid-induced derangements in thyroid function since majority of these patients are maintained on this medication for the control of their rheumatic disorder. Among the 7 patients with subclinical hypothyroidism, 3 were noted to have urinary iodide < 100 µg/L and the only patient with clinical hypothyroidism had urinary iodide level at 70 µg/L. Six patients had subclinical hyperthyroidism. Their thyroid function test profile may be due to the effect of steroids on the serum TSH. The single patient with clinical hyperthyroidism, probably iodide-induced, had urinary iodide level at 553 µg/L.
We found a significant association between duration of the autoimmune rheumatic disorder and autoimmune thyroid disease. A shorter duration of ARD (mean duration of 59 months compared to 88 months) was associated with ATD. It has been hypothesized that there is slow universal progression of the autoimmune process so that patients develop the disease over time. Thus, we expect that a longer disease duration would be associated with ATD. However, the opposite was observed in this study.
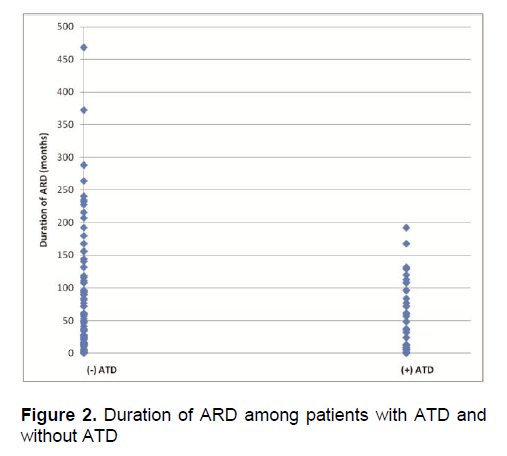
There was a previous observation that serological status of some SLE patients fluctuates and patients may become thyroid antibody negative with time. This subgroup is unlikely to develop clinical thyroid disease.6 This may explain the finding in our study that patients with longer duration of ARD were less likely to have coexisting ATD. But this needs to be proven by prospective studies considering that there was considerable overlap in the ARD duration among patients with ATD and without ATD (Figure 2). We did not find a significant association with the other clinical features of our subjects although there was an almost significant association observed for the presence of goiter. Features considered high risk for thyroid dysfunction in SLE patients include female sex, anti-TPO positivity, and a hypoechoic small thyroid on ultrasound.7 Subjects with these features should have thyroid function follow-up and appropriate treatment in due course.
Click here to download Figure 2
Figure 2. Duration of ARD among patients with ATD and without ATD
Data support the view that patients with systemic autoimmune diseases should be screened for the coexistence of thyroid disorders and that intermittent screening may be warranted.2-4, 7 Antonelli et al7 suggested that thyroid function and anti-TPO should be tested and ultrasonography should be performed as part of the clinical profile of SLE patients. In their study, the presence of hypoechoic thyroid and dyshomogenous echogenicity on ultrasound was used to determine thyroid autoimmunity in patients with negative antibodies. They recommended that those with high risk profile (women, positive anti-TPO, hypoechoic, and small thyroid) should have thyroid function follow-up. Appenzeller and colleagues8 concluded in their study that since symptoms of SLE and thyroid disease can be similar, SLE patients should routinely be investigated for autoimmune thyroid disease. Pyne and Isenberg recommend intermittent biochemical screening of thyroid function in patients with SLE, particularly if they are known to have thyroid antibodies, to identify clinical or subclinical thyroid disease. Subclinical thyroid dysfunction is associated with abnormality in the lipid profile, neuropsychiatric behavior, cardiac function and even cardiovascular risk. Hypothyroidism may be independently associated with higher cardiovascular risk in women with RA, as stated in the article by Goncalves et al.14
Autoimmune thyroid disease commonly occurs in patients with autoimmune rheumatic disorders, with a prevalence of 21.94% in this patient population. As such, it is important to consider screening these patients for a coexistent thyroid disease early in the course of their rheumatologic condition to help prevent the complications associated with thyroid dysfunction and to avoid adding to the morbidity of the existing autoimmune rheumatic disorder.
We recommend that a prospective study be done to follow-up the patients with antibody positivity but no derangement in thyroid function to determine when they will develop thyroid dysfunction.
This study was supported by a Research Grant in Endocrinology of the Philippine Society of Endocrinology and Metabolism.
We would also like to acknowledge Ms. Mercy Parazo for her statistical analysis.
1. Boelaert K, Newby P, Simmonds M, et al. Prevalence and relative risk of other autoimmune diseases in subjects with autoimmune thyroid disease. American Journal of Medicine. 2010; 123:183.e1-183.e9.
2. Weetman P. Non-thyroid autoantibodies in autoimmune thyroid disease. Best Practice & Research Clinical Endocrinology & Metabolism. 2005; 19(1):17-32.
3. Biro E, Szekanecz Z, Czirjak L, et al. Association of systemic and thyroid autoimmune diseases. Clinical Rheumatology. 2006; 25(2):240-245.
4. Lazurova I, Benhatchi K, Rovensky J, et al. Autoimmune Thyroid Disease and Autoimmune Rheumatic Disorders: A Two-sided Analysis. Annals of the New York Academy of Sciences. 2009; 1173:211-216.
5. Porkodi R, Ramesh S, Mahesh A, et al. Thyroid dysfunction in systemic lupus erythematosus and rheumatoid arthritis. J Indian Rheumatol Assoc. 2004; 12:88-90.
6. Pyne D, Isenberg DA. Autoimmune thyroid disease in systemic lupus erythematosus. Ann Rheum Dis. 2002; 61:70-72.
7. Antonelli A, Fallahi P, Mosca M, et al. Prevalence of thyroid dysfunctions in systemic lupus erythematosus. Metabolism Clinical and Experimental. 2010; 59:896-900.
8. Appenzeller S, Pallone A, Natalin R, et al. Prevalence of thyroid dysfunction in systemic lupus erythematosus. Journal of Clinical Rheumatology. 2009; 15(3):117-119.
9. Atzeni F, Doria A, Ghirardello A, et al. Anti-thyroid antibodies and thyroid dysfunction in rheumatoid arthritis: Prevalence and clinical value. Autoimmunity. 2008; 41(1):111-115.
10. Boey ML, Fong PH, Lee JSC, et al. Autoimmune thyroid disorders in SLE in Singapore. Lupus. 1993; 2:51-54.
11. Park DJ, Cho CS, Lee SH, et al. Thyroid disorders in Korean patients with systemic lupus erythematosus. Scandinavian Journal of Rheumatology. 1995; 24(1):13-17.
12. Tsai RT, Chang TC, Wang CR, et al. Thyroid disorders in Chinese patients with systemic lupus erythematosus. Rheumatology International. 1993; 13(1):9-13.
13. Soldevilla HF, Navarra SV. Thyroid disorders in Filipino patients with systemic lupus erythematosus. University of Santo Tomas Hospital, Manila. (Unpublished).
14. Goncalves F, Taciana C, Ranza R, et al. Autoimmune thyroiditis and rheumatoid arthritis: Is there really an association? The Endocrinologist. 2009; 19(1):31-34.
15. Ladenson P, Singer P, Ain K, et al. American Thyroid Association Guidelines for Detection of Thyroid Dysfunction. Arch Intern Med. 2000; 160:1573-1575.
16. Fauci A, Braunwald E, Kasper D, et al, eds. Harrison’s Principles of Internal Medicine, 17th edition. USA: McGraw-Hill, 2008.
17. 1980 Criteria for the Classification of Systemic Sclerosis. http://www.rheumatology.org/practice/clinical/classification/systsclr.asp. Accessed August 2010.
18. Vanderpump MP, Tunbridge WM, French JM, et al. The incidence of thyroid disorders in the community: A twenty-year follow-up of the Whickham Survey. Clin Endocrinol (Oxf). 1995; 43:55-68.
Articles and any other material published in the JAFES represent the work of the author(s) and should not be construed to reflect the opinions of the Editors or the Publisher.
Authors are required to accomplish, sign and submit scanned copies of the JAFES Declaration that the article represents original material that is not being considered for publication or has not been published or accepted for publication elsewhere.
Consent forms, as appropriate, have been secured for the publication of information about patients; otherwise, authors declared that all means have been exhausted for securing such consent.
The authors have signed disclosures that there are no financial or other relationships that might lead to a conflict of interest. All authors are required to submit Authorship Certifications that the manuscript has been read and approved by all authors, and that the requirements for authorship have been met by each author.