A 22-year old female (patient A) (Fig.1) (Fig.2) born from non-consanguineous marriage and two siblings from a separate family, 10-year-old boy (patient B) (Fig.3) and 15-year-old girl (patient C) (Fig.3), born from consanguineous marriage had common features of weight gain, postaxial (ulnar) polydactyly, speech delay, developmental delay with learning difficulties and progressive deterioration of vision since early childhood. Click here to download Figure 1
Figure 1. Photograph of patient A showing an overweight female.
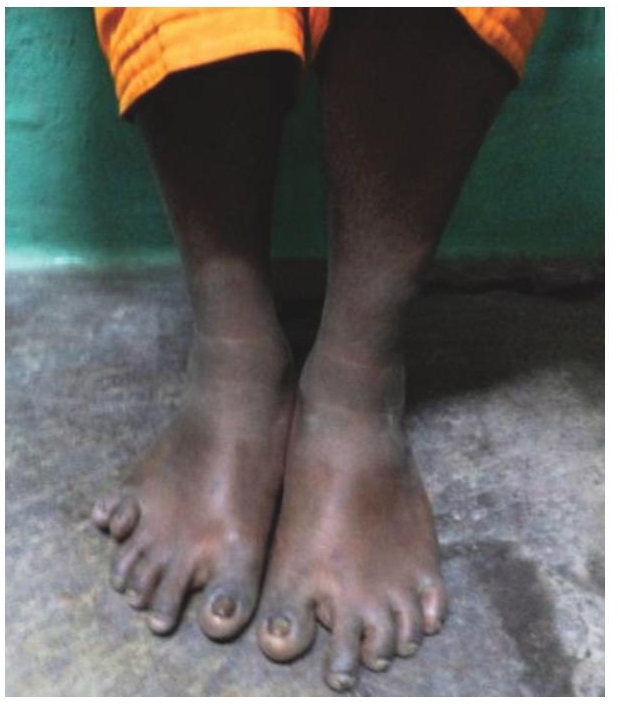
Click here to download Figure 2
Figure 2. Postaxial polydactyly in patient A.
Click here to download Figure 3
Figure 3. Photograph showing the two overweight siblings (patients B and C) with postaxial polydactyly.

The boy (patient B) had ataxia; body mass index (BMI) of 23.5 kg/m2 (>95th centile) with phallic length of 5 cm and testis measuring 3 cc bilaterally. Both grls (patients A and C) also had higher BMI [first patient: 27.4kg/m2 and third patient: 26.8 kg/m2 (>95th centile)]; regular menstrual cycles and normal secondary sexual characteristics.
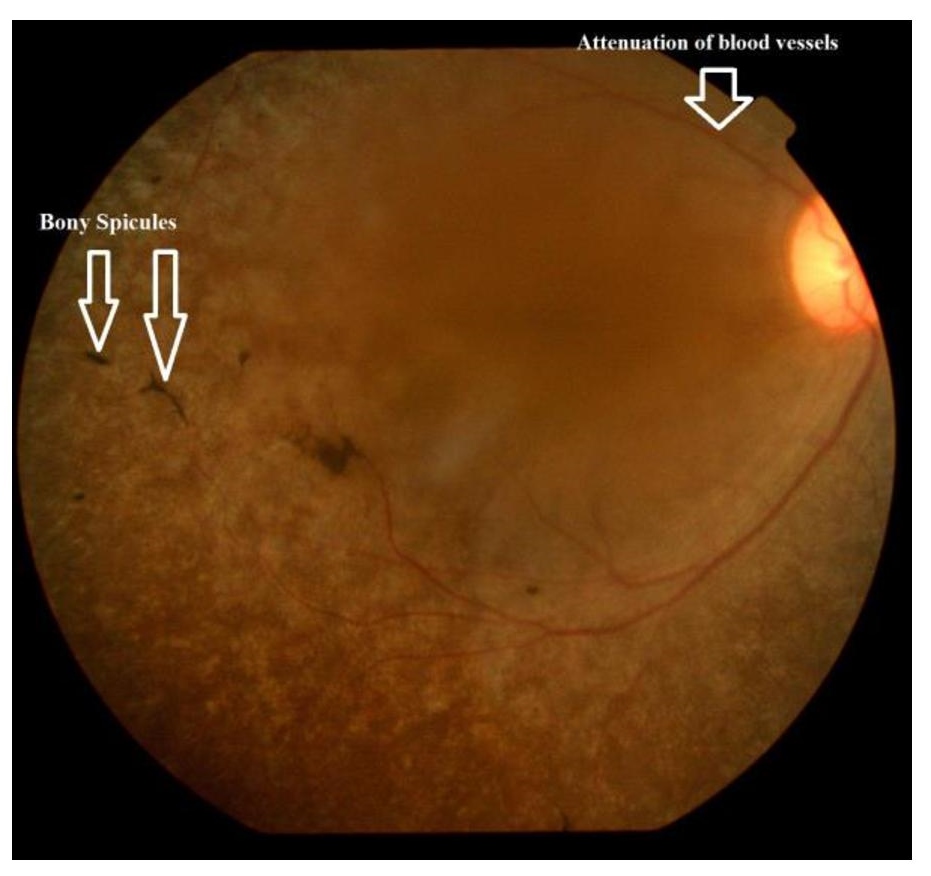
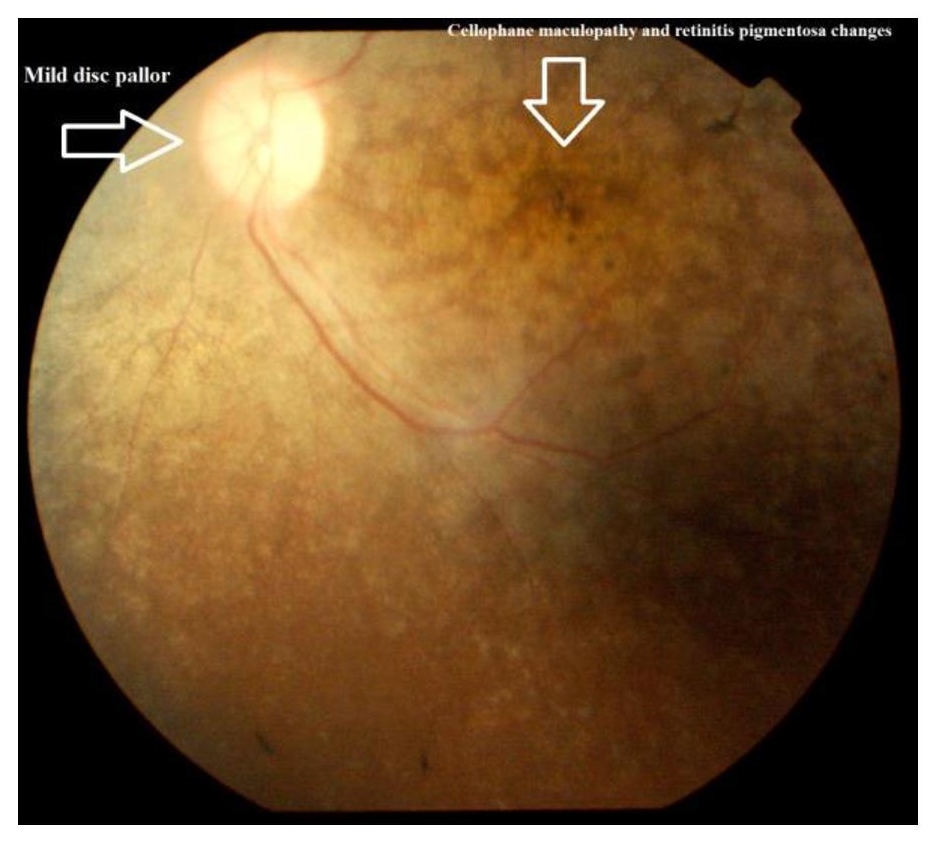
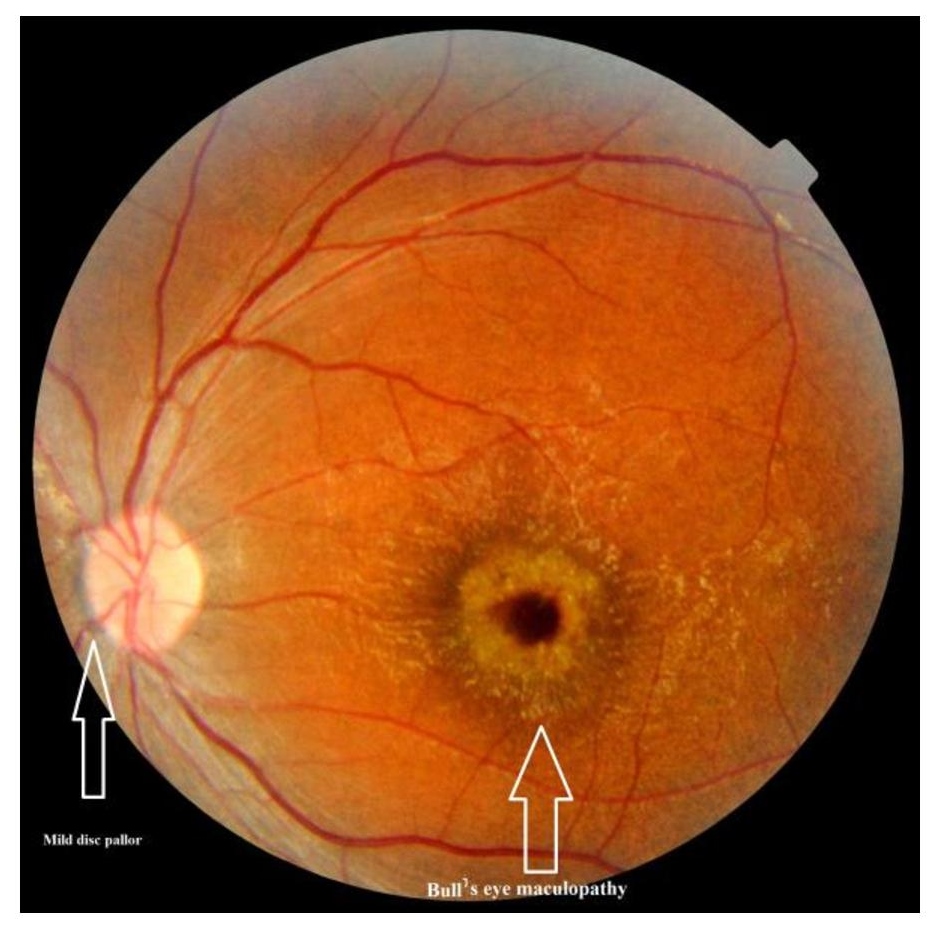
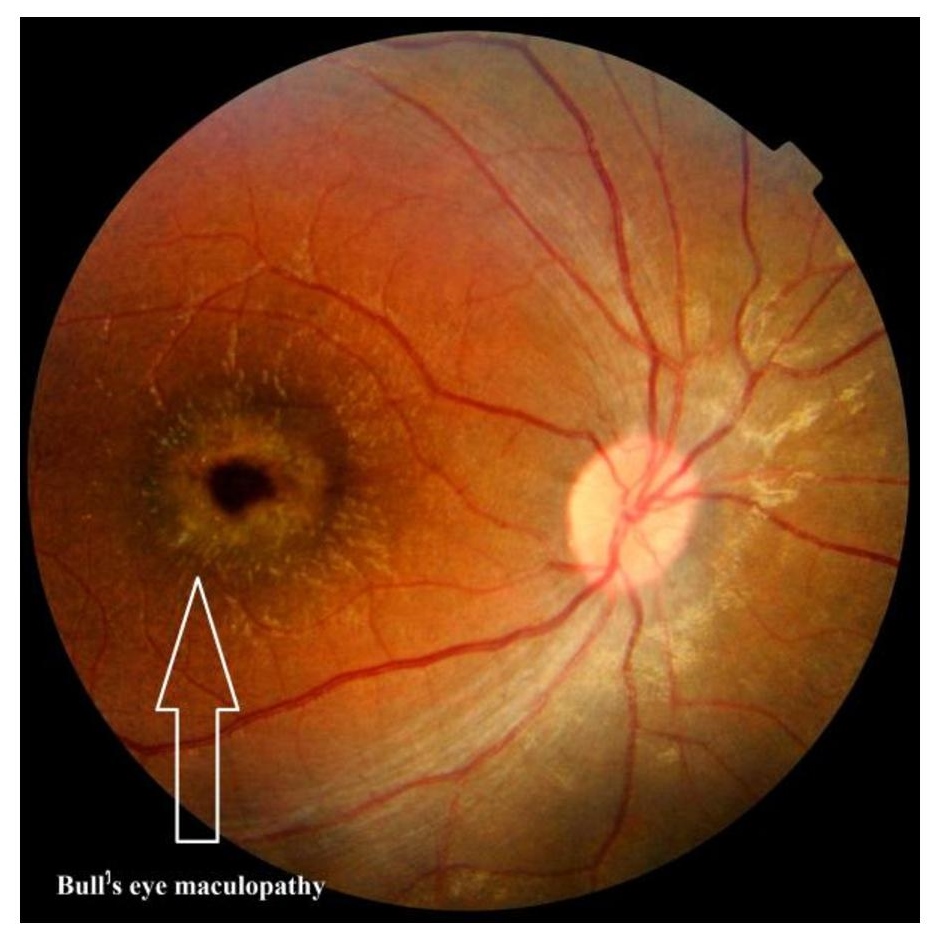
Fundus examination: Patient A: mild pallor of the disc, attenuation of retinal arterioles; cellophane maculopathy; few isolated bony spicules along the seminal blood vessels (fig.4)(Fig.5).
Click here to download Figure 4Figure 4. Fundus photograph of the right eye (patient A).
Click here to download Figure 5
Figure 5. Fundus photograph of the left eye (patient A).
Patient B: mild pallor of the disc; presence of internal limiting membrane folds surrounding the fovea; retinal pigment epithelial atrophy around the foveal and perifoveal zone resembling Bull's eye maculopathy (Fig.6)(Fig.7).
Click here to download Figure 6Figure 6. Fundus photograph of the left eye (patient B).
Click here to download Figure 7
Figure 7. Fundus photograph of the right eye (patient B).
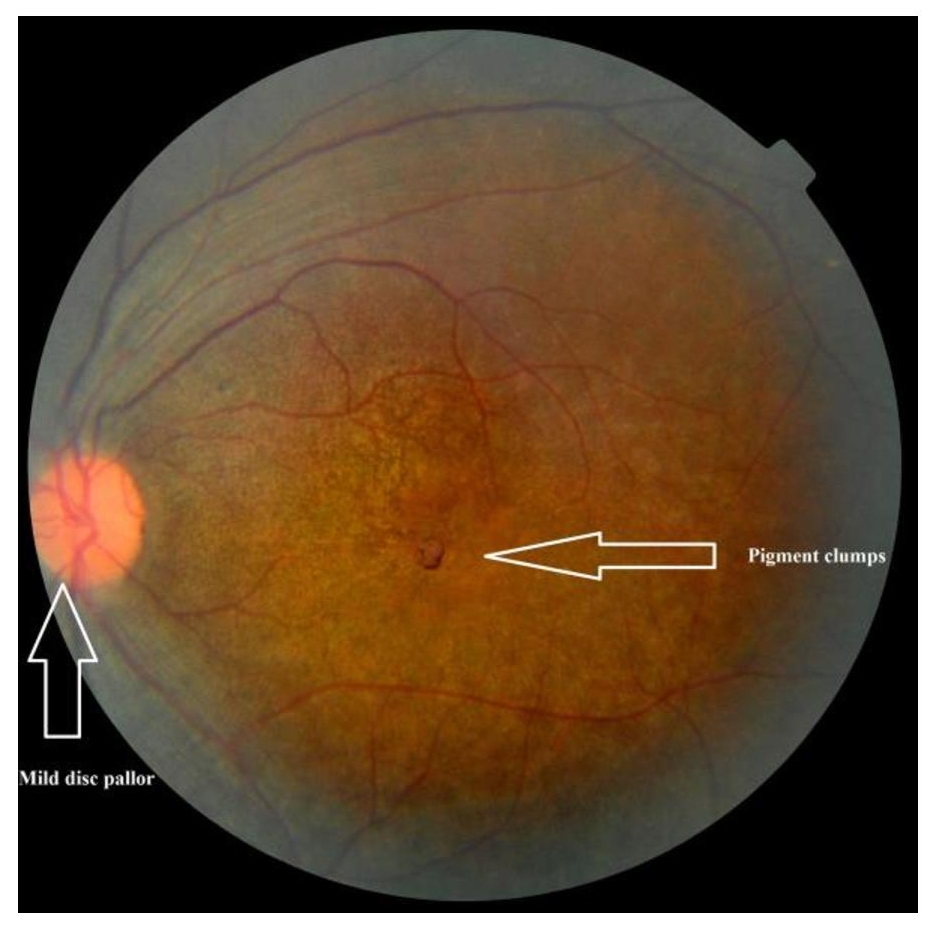
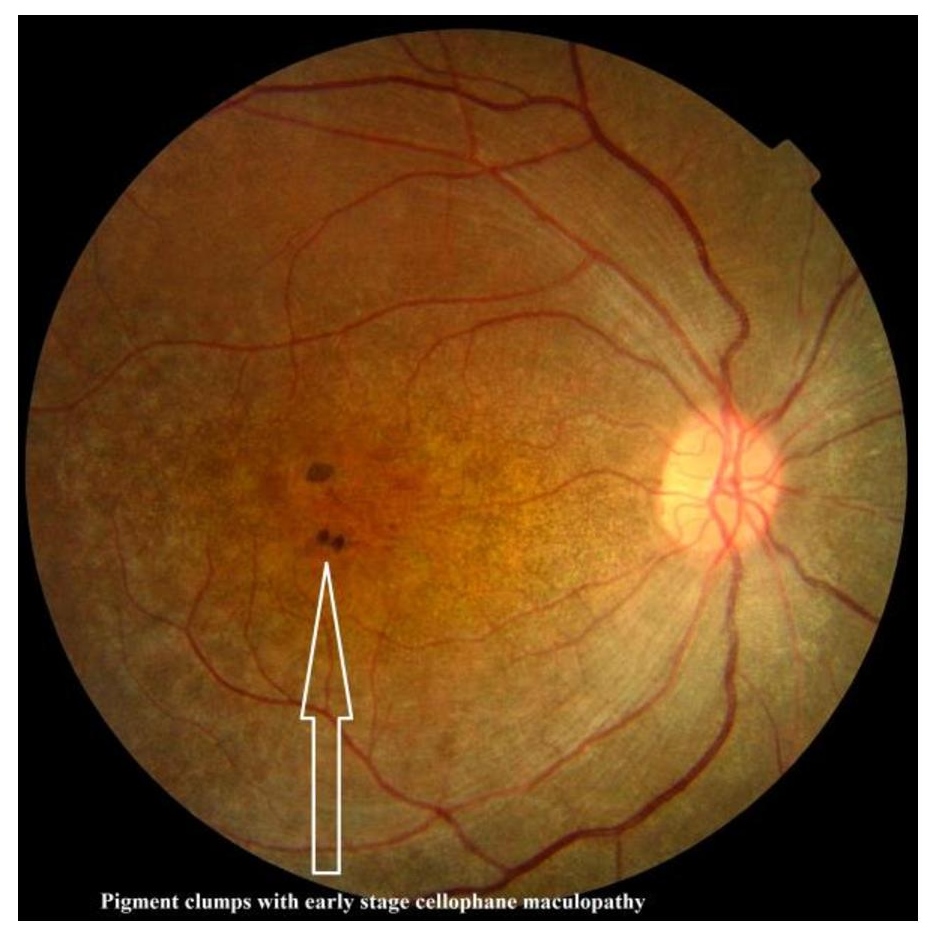
Patient C: mild pallor of the disc; attenuation of retinal arterioles; cellophane maculopathy with pigment clumps around the macula (Fig.8)(Fig.9). Biochemical investigations including correlated hormonal and lipid profile, ultrasound (USG) abdomen and echocardiography were non-contributory. Electroretinography and further investigations were refused by the patients' families.
Click here to download Figure 8Figure 8. Fundus photograph of the left eye (patient C).
Click here to download Figure 9
Figure 9. Fundus photograph of the right eye (patient C).
Based on the manifestation, the following differential diagnoses of syndromes associated with obesity were considered: Weiss syndrome, Biemond II syndrome, McKusick-Kauffman syndrome, Alstrom syndrome and Bardet-Biedl syndrome.1,2
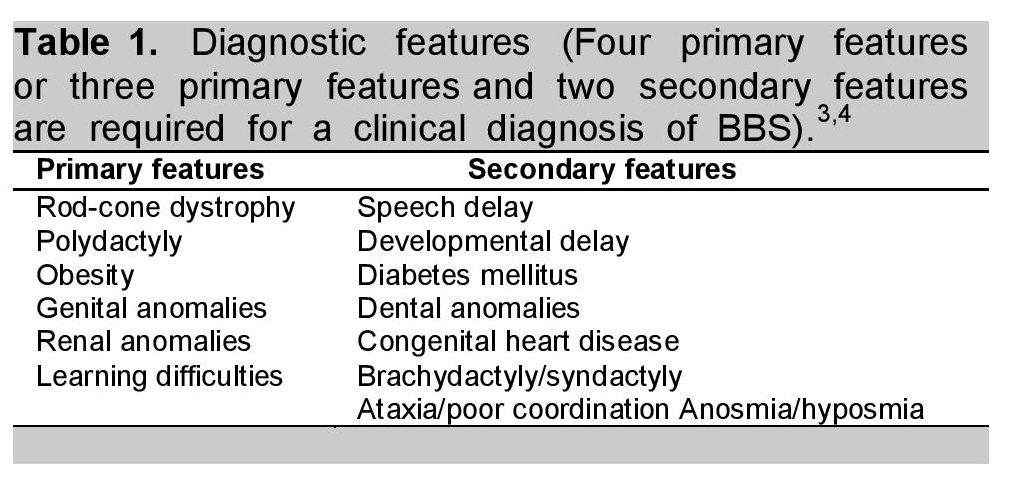
With characteristic clinical features, Bardet-Biedl syndrome (BBS) was diagnosed in our patients as per modified diagnostic criteria by Beales et al., (Table 1)3,4 and other possibilities were ruled out. The inheritance of BBS is usually considered autosomal recessive although this was absent in our first case. The diagnosis can be made based on clinical features and phenotype evolves variably in different patients.
Click here to download Table 1Table 1. Fundus photograph of the right eye (patient C).
Hypogonadism in BBS patients may manifest as delayed puberty or hypogenitalism in males and genital abnormalities in female;2,5,6 although this was absent in our cases at the time of presentation.
Bardet-Biedl syndrome is also a genetic form of obesity probably caused by mutations in any of at least 12 genes with increased risk of diabetes, and it is distinct from nonsyndromic obesity.3-6 Feuillan et al., found that patients with BBS had higher leptin than expected for their degree of adiposity, consistent with the notion that ciliopathy-induced leptin signaling dysfunction is associated with leptin resistance. These BBS patients also had predisposition for metabolic complications, including hypertension and hypertriglyceridemia.7 Apart from obesity, our cases (diagnosed in late childhood to adolescence) are probably still in the evolving phase of other metabolic and endocrine complications which we will follow up and manage accordingly. The ocular phenotypes in BBS2, BBS3 and BBS4 genotypes were reported to be early and severe.8 However, in our cases, fundus findings varied even within the same family. This spectrum of findings may further elucidate the evolving pathogenesis of BBS.
1. Schachat A, Maumenee IH. Bardet-Biedl syndrome and related disorders. Arch Ophthalmol.1982;100:285-288. http://dx.doi.org/ 10.1001/archopht.1982.01030030287011.
2. Deveault C, Billingsley G, Duncan JL et al: BBS genotype-phenotype assessment of a multiethnic patient cohort calls for a revision of the disease definition. Hum Mutat.2011;32:610-619. http://dx.doi.org/10.1002/humu.21480.
3. Beales PL, Elcioglu N, Woolf AS, Parker D, Flinter FA. New criteria for improved diagnosis of Bardet-Biedl syndrome: Results of a population survey. J Med Genet.1999;36:437-446.
4. Beales PL. Lifting the lid on Pandora's box: The Bardet-Biedl syndrome. Curr Opin Genet Dev.2005;15:315-323. http://dx.doi.org/10.1016/ j.gde.2005.04.006.
5. Elizabeth Forsythe and Philip L Beales. Bardet-Biedl syndrome. Eur J Hum Genet. 2013;21:8-13. http://dx.doi.org/10.1038/ejhg.2012.115.
6. Rooryck C, Lacombe D. Bardet-Biedl syndrome. Ann Endocrinol (Paris).2008; 69:463-471. http://dx.doi.org/10.1016/j.ando.2008.10.001. Penelope P. Feuillan, David Ng, Joan C. Han, Julie C. Sapp, Katie Wetsch, Emma Spaulding et al. Patients with Bardet-Biedl syndrome have hyperleptinemia suggestive of leptin resistance. J Clin Endocrinol Metab. 2
7. Penelope P. Feuillan, David Ng, Joan C. Han, Julie C. Sapp, Katie Wetsch, Emma Spaulding et al. Patients with Bardet-Biedl syndrome have hyperleptinemia suggestive of leptin resistance. J Clin Endocrinol Metab. 2011;96(3):528-535. http://dx.doi.org/10.1210/ jc.2010-2290.
8. Heon E, Westall C, Carmi R et al. Ocular phenotypes of three genetic variants of Bardet-Biedl syndrome. Am J Med Genet A.2005;132:283-287. http://dx.doi.org/10.1002/ajmg.a.30466.
Authors are required to accomplish, sign and submit scanned copies of the JAFES Declaration that the article represents original material that is not being considered for publication or has not been published or accepted for publication elsewhere.
Consent forms, as appropriate, have been secured for the publication of information about patients; otherwise, authors declared that all means have been exhausted for securing such consent.
The authors have signed disclosures that there are no financial or other relationships that might lead to a conflict of interest. All authors are required to submit Authorship Certifications that the manuscript has been read and approved by all authors, and that the requirements for authorship have been met by each author.