The International Diabetes Federation projects that 592 million individuals will have diabetes by the year 2035.1,2 The prevalence of type 2 Diabetes Mellitus (DM) is also rising in younger individuals presumably because of increasing obesity and reduced activity levels as countries become more industrialized.3
The association between thyroid dysfunction and DM has long been recognized. Thyroid hormones are insulin antagonists; both insulin and thyroid hormones are involved in cellular metabolism and excess and deficit of any one can result in functional derangement of the other . As diabetes is a major public health problem, any disorder that may even be weakly associated with it merits special attention.
Very few studies are reported regarding the relationship of thyroid dysfunction in type 2 DM in young patients. The control of hyperglycaemia in the presence of underlying thyroid dysfunction, even subclinical, poses problems. Correction of thyroid dysfunction may help improve metabolic outcome in type 2 DM patients. As such, thyroid dysfunction and Type 2 DM may be interlinked. Currently there are no internationally accepted guidelines for screening of thyroid dysfunction in Type 2 DM patients. This study therefore is designed to inform the burden of dual pathological prevalence of thyroid dysfunctions in young (less than 40 years) type 2 DM patients.
Objectives- To assess the thyroid abnormalities in diabetic subjects with or without symptoms of thyroid dysfunction;
- To assess the prevalence of thyroid dysfunction based on biochemical and/or clinical features;
- To assess the anti TPO positivity in patients with thyroid dysfunction.
The study includes type 2 diabetics of age less than 40 years. Total of 120 patients were selected who were diagnosed as having type 2 DM in accordance with ADA criteria and evaluated with thyroid function tests (FT4, TSH).
Exclusion Criteria- Type 1 DM
- Type 2 DM above 40 yrs of age
- Gestational DM
- Proven thyroid disorder and under treatment
- Very sick or critically ill patients
- Patients who had undergone surgery of the thyroid gland
- Patients who had exposure to radiation of the thyroid gland
- Patients with drug-induced hyperglycemia
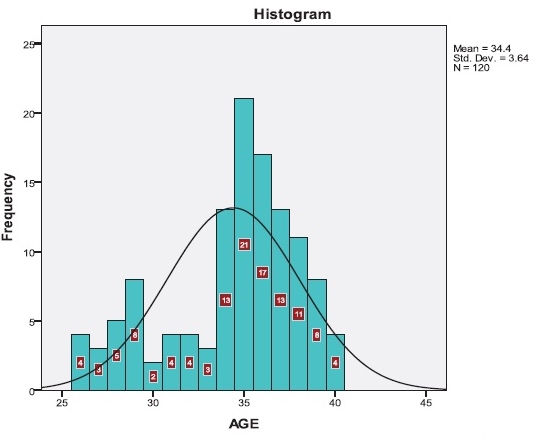
Of the 120 patients, 81 were males (67.5%) and 39 were females ( 32.5%). Their average age is 35 years old. The youngest subject in our study was 26 years old (Figure 1).
Click here to download Figure 1Figure 1. Distribution of age in the study population (n=120).
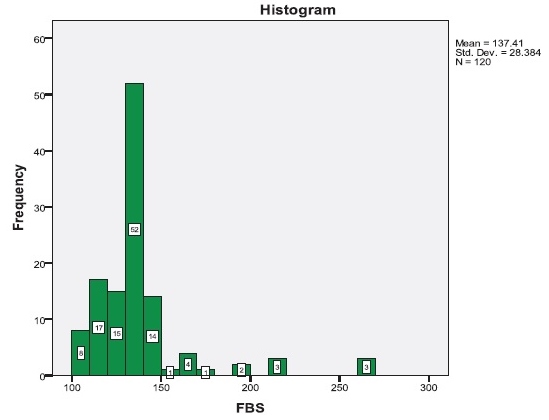
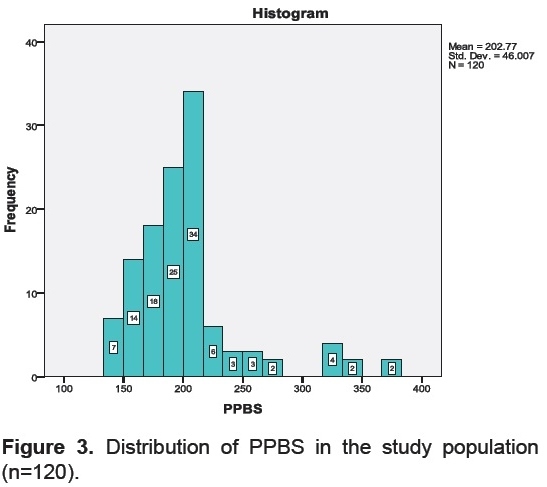
Average FBS level in recently diagnosed Type 2 DM population was 137 mg/dl and 95% of the population falls within the range of 130 mg/dl to 161 mg/dl (Figure 2). Average postprandial blood sugar (PPBS) in this population was 223 mg/dl with 95% of them between 190-234 mg/dl (Figure 3).
Click here to download Figure 2Figure 2. Distribution of FBS in the study population (n=120).
Click here to download Figure 3
Figure 3. Distribution of PPBS in the study population (n=120).
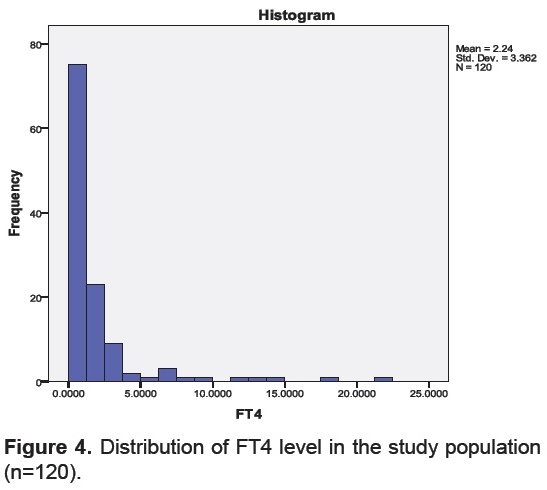
HbA1c prevalence in 95% ( 2 S.D.) of the population was within 7.5 to 8%. Normal range for serum FT4 level is 0.7-1.24 μg/dl (standardized for all values). Figure 4 and Figure 5 showed the distribution of FT4 and TSH level in the study population.
Click here to download Figure 4Figure 4. Distribution of FT4 level in the study population (n=120).
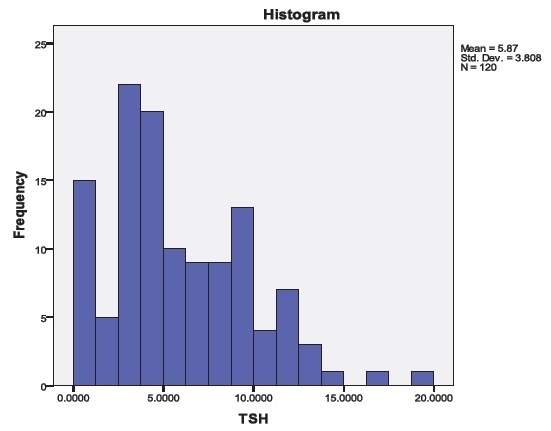
Click here to download Figure 5
Figure 5. Distribution of TSH level in the study population (n=120).
Click here to download Figure 1
Figure 1. Frequency distribution of subacute thyroiditis patients by year, 2007-2013.
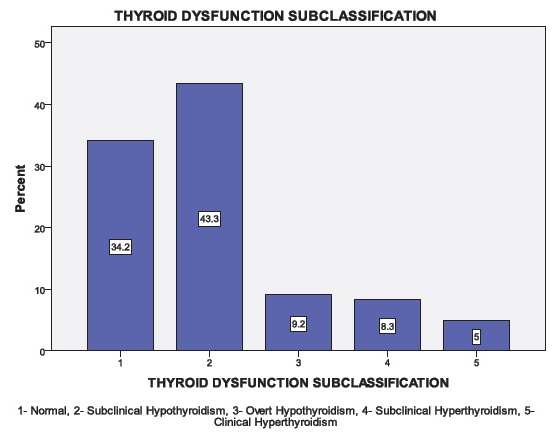
The study revealed that 65.8% of patients (79 out of 120) have biochemical features of thyroid dysfunction. Out of the 79 patients, 63 patients have biochemical features of hypothyroidism (79.74% of patients with thyroid dysfunction and 52.5% of the total population). 16 patients have biochemical features suggestive of hyperthyroidism (20.25% of patients with thyroid dysfunction and 13.33% of the total population). Further analysis showed that 43.33% had subclinical hypothyroidism (defined by no symptoms or no clinical features of hypothyroidism but with TSH level in the range of above 5 miu/ml but below 10 miu/ml with normal FT4 level), 9.2% had overt hypothyroidism (either with clinical features or TSH >10 miu/ml or FT4 below normal), 8.3% had subclinical hyperthyroidism (with only low level of TSH <0.34 miu/ml) and 5% patients had overt hyperthyroidism ( with clinical features or FT4 level above normal range along with low TSH) (Figure 6).
Click here to download Figure 6Figure 6.Thyroid dysfunction in the study population (n=120).
To know the prevalence of autoimmunity in thyroid dysfunction, anti-TPO test was done. The study revealed that 22 patients out of the 79 patients with thyroid dysfunction were positive for anti -TPO antibodies (27.84% of total thyroid abnormality), whereas 57 patients with thyroid dysfunction were anti-TPO negative (72.15%). 7 patients without any thyroid dysfunction showed anti-TPO positivity (17.07%).
India will have 109 million diabetics by 2035 as projected by International Diabetes Federation.2 Sequential surveys from India indicate that the prevalence of diabetes has risen steadily in the last few decades and more so in younger people.4-7
In our study, the average age of the study population was 35 years old which is a great burden for the society. Our study results are similar to several recent studies8 and previous study of our own by Mukherjee S et al9 in the general population . The mean age of detection of type 2 DM is 35 years in this study. This study reflects a large number of type 2 DM patients with early onset of their disease in contrast to the National Urban Diabetes Survey, carried out in six cities in 2001 in India.7 However, recent studies like the Chennai Population Study (CUPS) showed similar prevalence in younger generation.10
The high fasting blood sugar level in our study reflects higher level of abnormal metabolic status in this part of India which causes more problem in maintaining normoglycaemia in younger individuals. The average PPBS in this study was almost similar to previous studies.9 Distribution of HbA1c in this study is consistent with several studies.11 Our study revealed FT4 level has little value in screening for thyroid dysfunction as most of the patients were found to have normal levels of FT4. But TSH level is significantly abnormal in large number of patients reflecting underlying thyroid abnormality in majority of the sample population, which is similar to previous studies.12
This study shows that 65.8% of this young diabetic population had thyroid dysfunction which is much higher than several previous studies, though it was in accordance with Mukherjee et al reported from eastern India.9 This study showed much higher rate of thyroid dysfunction compared to several previous studies which showed lesser prevalence of this association and varied from 1.7% to 23% in different populations.13-16
Studies on pediatric population in India had shown higher prevalence of subclinical hypothyroidism (31.2%).17 A very high prevalence has also been noted outside India, from Nigeria, (46.5%).18 Subclinical hypothyroidism is the most common disorder in our study (43.33%) which is similar to several studies reported.19-22
This study, is the first of its kind in Eastern India, showing very high prevalence of thyroid dysfunction in younger diabetics. As diabetes mellitus is currently increasingly diagnosed in the younger age group, this association has gained a new implication.
The causal association between high prevalence of abnormal thyroid hormone levels in younger diabetics is not fully understood. In our study, very high occurrence of thyroid dysfunction in younger diabetic individuals suggests a dual pathologic prevalence where autoimmunity is playing probably a minor role as evident from previous discussion.
Different studies support a biologically plausible role for hypothyroidism increasing the risk of atherosclerotic cardiovascular disease. Type 2 DM is also an independent risk factor for atherosclerotic cardiovascular disease.
This study suggests routine evaluation for thyroid screening and treatment in younger diabetics in this part of the world to prevent diverse complications of the high dual pathologic prevalence.
1. Diabetes Mellitus, Alvin C Powers, Dan L Longo, Dennis L Kasper, et al, Harrison's Principle of Internal Medicine, 18th ed., Mc Graw Hill publication, p. 2968.
2. International Diabetes Federation. Diabetes Atlas , 6th edn. 2013, p. 34. 3. Chan JC, Malik V, Jia W, Kadowaki T, Yajnik CS, Yoon KH, et al. Diabetes in Asia: Epidemiology, risk factors, and pathophysiology. JAMA. 2009;301(20):2129-40. http://dx.doi.org/10.1001/jama.2009.726. 4. Ahuja M. Epidemiological studies on diabetes mellitus in India. In: Ahuja M. Epidemiology of diabetes in developing countries. New Delhi: Interprint, 1979, pp. 29-38. 5. Verma NP, Mehta SP, Madhu S, Mather HM, Keen H. Prevalence of known diabetes in an urban Indian environment: The Darya Ganj diabetes survey. Br Med J (Clin Res Ed). 1986;293:423-424. http://dx.doi.org/10.1136/bmj.293.6544.423. 6. Ramachandran A, Snehalatha C, Dharmaraj D, Viswanathan M. Prevalence of glucose intolerance in Asian Indians: Urban-rural difference and significance of upper body adiposity. Diabetes Care. 1992;15(10):1348-55. http://dx.doi.org/10.2337/diacare.15.10.1348. 7. Ramachandran A, Snehalatha C, Kapur A, Vijay V, Mohan V, Das AK, et al. High prevalence of diabetes and impaired glucose tolerance in India: National Urban Diabetes Survey. Diabetologia. 2001;44(9):1094-1101. http://dx.doi.org/10.1007/s001250100627. 8. Palma CCSSV, et al. Prevalence of thyroid dysfunction in patients with diabetes meelitus. Diabetol Metab Syndr. 2013;5:58. http://dx.doi.org/10.1186/1758-5996-5-58. 9. Mukherjee S, Datta S, Datta P, Mukherjee AK, Maisnam I. A study of prevalence of primary hypothyroidism in recently diagnosed type 2 diabetes mellitus in a tertiary care hospital. Int J Sci Rep. 2015;1(2):105-112. http://dx.doi.org/10.18203/issn.2454-2156.IntJSciRep20150216. 10. Mohan V, Deepa M, Anjana RM, Lanthorn H, Deepa R. Incidence of diabetes and pre - diabetes in a selected urban south Indian population (CUPS - 19). J Assoc Physicians India. 2008;56:152-157. 11. Uppal V, Vij C, Bedi GK, Vij A, Banerjee BD. Thyroid disorders in patients of type 2 diabetes mellitus. Indian J Clin Biochem. 2013;28(4):336-41. http://dx.doi.org.10.1007/s12291-012-0293-9. 12. Celani MF, Bonati ME, Stucci N. Prevalence of abnormal thyrotropin concentrations measured by a sensitive assay in patients with type 2 diabetes mellitus. Diabetes Res. 1994;27(1):15-25. 13. Ganz K, Kozak GP. Diabetes mellitus and primary hypothyroidism. Arch Intern Med. 1974;134(3):430-32. http://dx.doi.org/10.1001/archinte.1974.00320210040005. 14. Hecht A, Gershberg H. Diabetes mellitus and primary hypothyroidism. Metabolism. 1968;17(2):108-13. http://dx.doi.org/10.1016/0026-0495(68)90136-4. 15. Perros P, McCrimmon RJ, Shaw G, Frier BM. Frequency of thyroid dysfunction in diabetic patients: Value of annual screening. Diabet Med. 1995;12(7):622-27. http://dx.doi.org/10.1111/j.1464-5491.1995.tb00553.x. 16. Hage M, Zantout MS, Azar ST. Thyroid disorders and diabetes mellitus. J Thyroid Res. 2011;2011. http://dx.doi.org/10.4061/2011/439463. 17. Toteja GS, Singh P, Dhillon BS, Saxena BN. Iodine deficiency disorders in 15 districts of India. Indian J Pediatr. 2004;71(1):25-8. http://dx.doi.org/10.1007/BF02725651. 18. Udiong CEJ, Udoh AE and Etukudoh ME. Evaluation of thyroid function in diabetes Mellitus in Calabar, Nigeria. Indian J Clin Biochem. 2007;22(2)74-8. http://dx.doi.org/10.1007/BF02913318. 19. Pimenta WP, Mazeto GM, Callegaro CF, Shibata SA, Marins LV, Yamashita S, et al. Thyroid disorders in diabetic patients. Arq Bras Endocrinol Metabol. 2005;49:234-40. 20. Hector-Eloy Tamez-Pérez Esteban Martínez, Dania L, et al. The rate of primary hypothyroidism in diabetic patients is greater than in the non-diabetic population. An observational study.Med Clin (Barc). 2011. 21. Smithson MJ. Screening for thyroid dysfunction in a community population of diabetic patients. Diabet Med.1998;15(2):148-50. http://dx.doi.org/10.1002/(SICI)1096-9136(199802)15:2<148::AID-DIA540>3.0.CO;2-H. 22. Suzuki Y, Nanno M, Gemma R, Tanaka I, Taminato T, Yoshimi T. The mechanism of thyroid hormone abnormalities in patients with diabetes mellitus. Nippon Niabunpi Gakki Zasshi. 1994;70(4):465-70. http://dx.doi.org/10.1507/endocrine1927.70.4_465.Authors are required to accomplish, sign and submit scanned copies of the JAFES Declaration that the article represents original material that is not being considered for publication or has not been published or accepted for publication elsewhere.
Consent forms, as appropriate, have been secured for the publication of information about patients; otherwise, authors declared that all means have been exhausted for securing such consent.
The authors have signed disclosures that there are no financial or other relationships that might lead to a conflict of interest. All authors are required to submit Authorship Certifications that the manuscript has been read and approved by all authors, and that the requirements for authorship have been met by each author.