Hemorrhage to the adrenal glands is a rare finding occurring more frequently in children than in adults. It is classically associated with meningococcal septicemia (Waterhouse-Friderichsen syndrome). In adults, it is mainly caused by trauma, surgical stress, anticoagulation therapy, or a tumor; however, spontaneous or idiopathic adrenal hemorrhage is extremely rare.1 Two mechanisms that have been proposed in the pathogenesis of idiopathic adrenal hematomas are stress and adrenal medullary venous thrombosis.2 In a review done by Vella et al at the Mayo Clinic, adrenal hemorrhages (AH) were classified into several categories: incidentaloma (28 cases), spontaneous AH (16 cases), AH associated with antiphospholipid- and heparin-associated thrombocytopenia (20 cases), postoperative AH (14 cases), AH associated with anticoagulation therapy (3 cases), AH associated with trauma (4 cases), and AH associated with severe stress or sepsis (56 cases).3 The clinical manifestations may vary depending on the amount of hemorrhage, its effect on hemodynamics and the rate of onset. A majority, however, may not have any symptom and the diagnosis may be incidentally discovered through imaging.1,4 This patient initially had an ultrasound to further investigate a palpable mass over the posterior right upper quadrant area which later revealed a complex mass in the region of the porta hepatis. An abdominal CT scan was done to further investigate the said mass and it showed a retroperitoneal mass with characteristics suggestive of an adrenal neoplasm. In these instances, hormonal work-up is warranted to determine functionality of the tumor in preparation for surgery, as well as to determine any particular hormone excess in an adrenocortical carcinoma. Histopathology remains to be the gold standard in the diagnosis.
A 72-year-old Filipino male retired lawyer sought consult at his physician's clinic for a routine check-up. On examination, a soft, non-tender mass was palpated over the posterior right upper quadrant area in the lumbar region measuring about 12 x 6 cm (l x w). Patient denied pain over the area of the mass; and there was no history of trauma. He had been experiencing intermittent episodes of generalized weakness and body malaise, and noted an approximate 10-pound weight loss over the past year but otherwise he was ambulant and maintained good functional capacity. The patient has had no previous surgery, no intake of any anti-platelets nor anti-coagulants. He has been diabetic for approximately 5 years with good control, maintained on metformin, acarbose and gliclazide. His hypertension is controlled with indapamide; dyslipidemia is managed with fibrates. Other medications include allopurinol for hyperuricemia, and nitrates for ischemic heart disease.
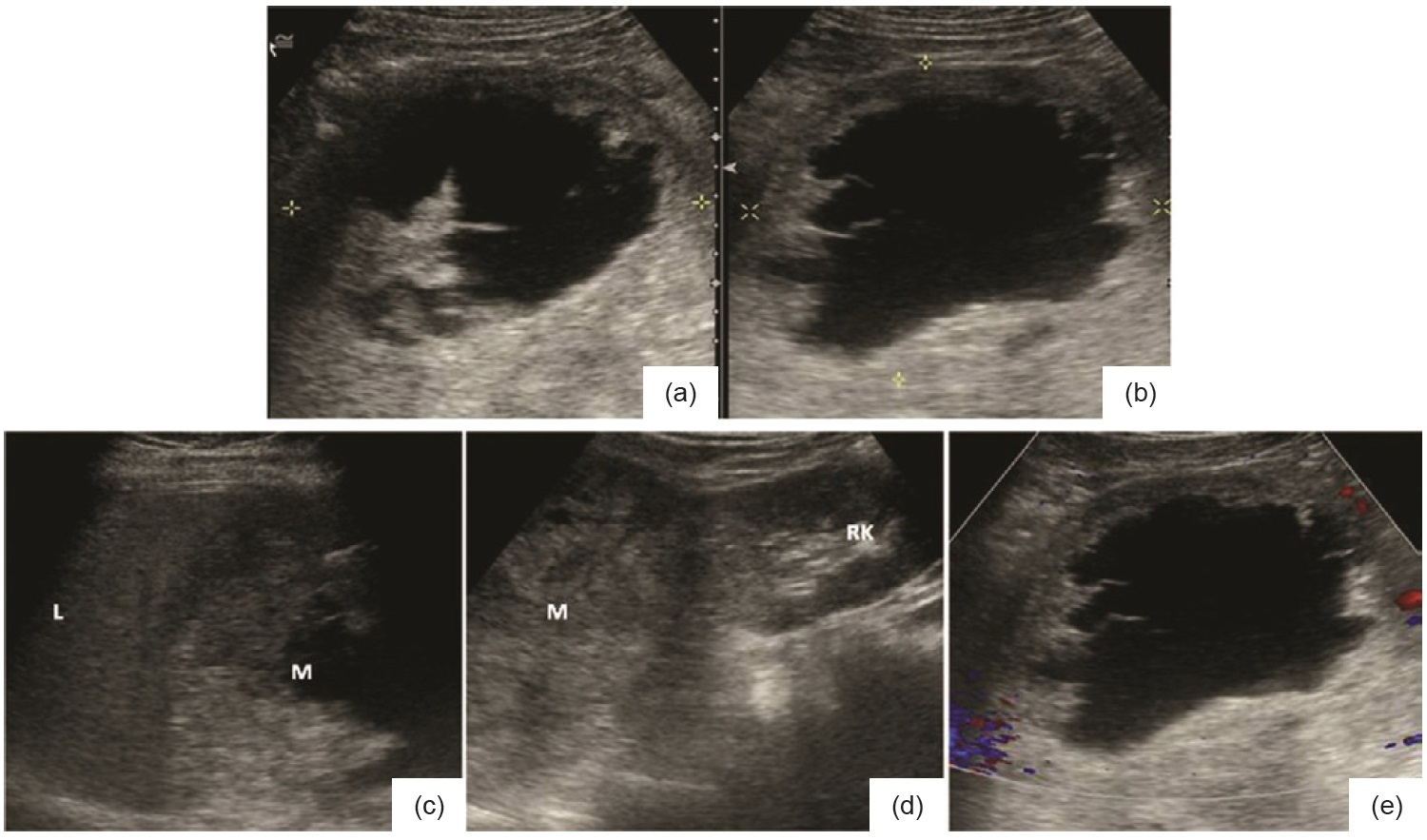
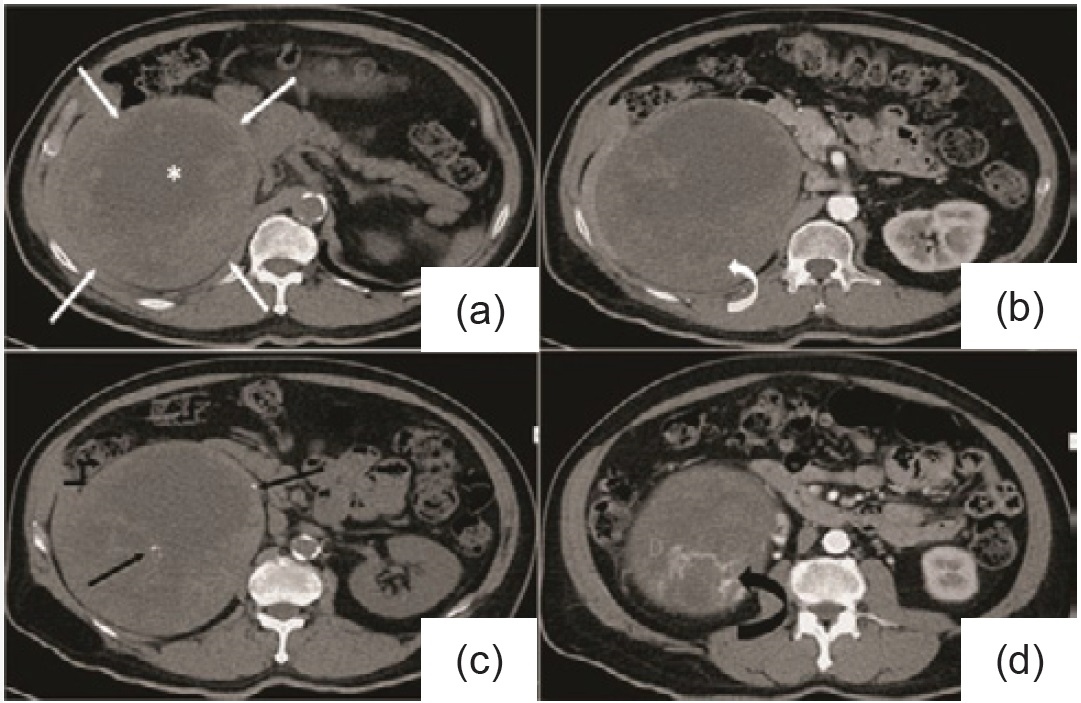
Initial consideration for the palpable mass was a lipoma. On ultrasound of the whole abdomen, there was note of a well-defined encapsulated heterogenous mass lesion with central cystic probably necrotic component at the region of the porta hepatis, measuring 11.32 x 11.43 x 10.89 cm. The said lesion appears to displace the right hepatic lobe superiorly and the right kidney inferiorly. Minimal peripheral vascularity is noted under color Doppler evaluation (Figure 1). With the abovementioned findings, a CT scan of the whole abdomen was subsequently done, revealing a large heterogeneous mass lesion with a central hypodense component (likely necrosis) centered in the right retroperitoneal region, with non-contrast Hounsfield units ranging from 15-40 HU (Figure 2a and 2b). It measures 14.2 x 12.5 x 14.7 cm in its maximal craniocaudal x width x anteroposterior dimensions. Neovascularities and small calcific components are identified within the said mass. It displaces the liver superiorly, the right kidney inferiorly, and also splays and compresses the right renal artery and vein. After correlating the ultrasound and CT scan findings, the primary consideration for this lesion was an adrenal neoplasm.
Click here to download Figure1Figure 1 a and b. Transverse and sagittal sonographic images revealing a complex mass at the region of the porta hepatis; c and d. Sagittal images showing superior displacement of the right hepatic lobe (L) and inferior displacement of the right kidney (RK) by the mass (M); e. Minimal peripheral enhancement detected under color Doppler imaging.
Click here to download Figure2
Figure 2. Axial non-contrast (a) and contrast-enhanced; b) CT images showing a large retroperitoneal mass (white arrows) with central hypodensity (*) and peripheral enhancement (curved white arrow); c. Non-contrast axial CT image showing punctate calcifications (black arrows); d. Contrast-enhanced axial CT image showing neovascularization (curved black arrow).
Click here to download Figure 2b
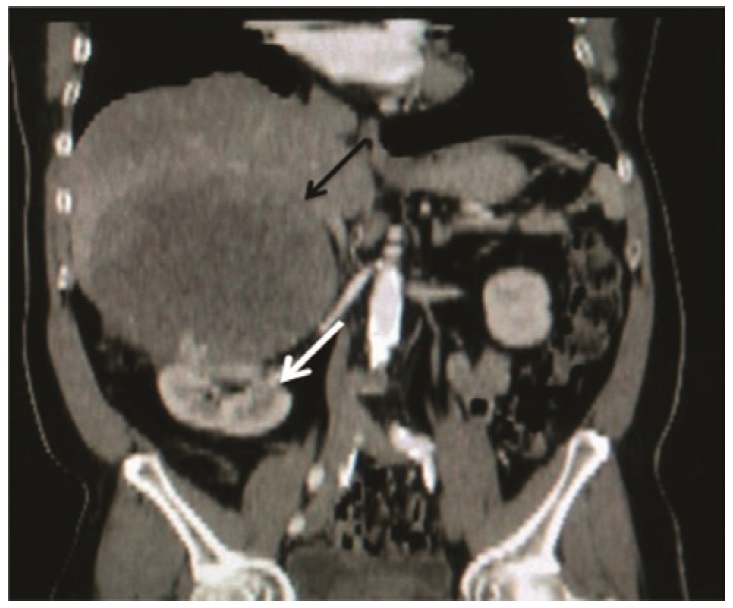
Figure 2b.Coronal contrast-enhanced CT image showing a suprarenal mass (black arrow) causing inferior displacement of the right kidney (white arrow)..
A hormonal work-up was subsequently done revealing a non-functioning adrenal mass. The results: Plasma Aldosterone-RIA 23.77 ng/dl (NV 3.0-35.5 ng/dl), Plasma Renin Activity 5.65 ng/ml/hr (0.5-1.9 ng/ml/hr supine; 1.9-6.0 ng/ml/hr upright), ARR: 4.207, Serum Cortisol (8 am): 15.7 ug/dl (NV 4.2-38.4), 24h urine metanephrine: 1.21 mg/24hr (NV up to 1 mg metanephrine/24 hr ); DHEA-S: 69.5 ug/dl (NV 33.6-249); Progesterone: 0.26 ng/ml (NV 0.2-1.31); Testosterone: 3.31 ng/ml (NV 1.95-11.38); Estradiol: 29 pg/ml (NV 20-77). A biopsy of the adrenal mass was then done however results were inconclusive. Other sources of a possible malignancy were investigated. Chest x-ray showed an atherosclerotic aorta, CEA was within normal range at 2.10 ng/ml NV 0-3). Prostatomegaly with hypodense nodules were likewise noted on CT scan hence a cysto-TURP was done later on with histopathology findings of a benign prostatic hyperplasia. The patient was not anemic with hemoglobin of 133 g/L and hematocrit of 0.39. The patient was hyponatremic at 127.8 meq/L and hypokalemic at 2.98 meq/L, which was attributed to the patient's anti-hypertensive medication that was then discontinued.
Click here to download Figure 3Figure 3a.(left). Gross appearance of the thinly encapsulated adrenal mass and measures 16.8 cm in greatest dimension. Figure 3b(right). Cross sections of the mass show yellow fibrinous solid areas with variably sized locules containing hemorrhagic fluid.

Exploratory laparotomy and resection of retroperitoneal mass on the right with cholecystectomy was done. Histopathologic findings revealed a diffuse adrenal hemorrhage, with no evidence of malignancy seen and chronic cholecystitis with cholelithiasis. Grossly, the specimen was described to be a large globular fluctuant mass weighing 1500 grams, measuring 16.8 x 14.0 x 9.0 cm.
The external capsule was thin, brown and smooth and covered with small fibrous tags. Cut sections of the mass showed a cream yellow granular to glistening cut surface with multiple locules measuring from 1.3 to 8.0 cm in diameter containing red brown watery to hemorrhagic fluid. The capsule measured 0.4 cm think. Microscopic examination showed mostly diffuse hemorrhage with fibrin surrounded by thin fibrous capsule. The adrenal gland was seen within the fibrous capsule compressed by the hemorrhage material. Delineation of the adrenal zones was not possible due to the compressive effect of the hemorrhage to the affected gland. Serum cortisol was repeated a year later and remained to be in the normal range at 12.6 ug/dl (NV 2.9-17.3). The patient continues to follow-up and is well 20 months post surgery.
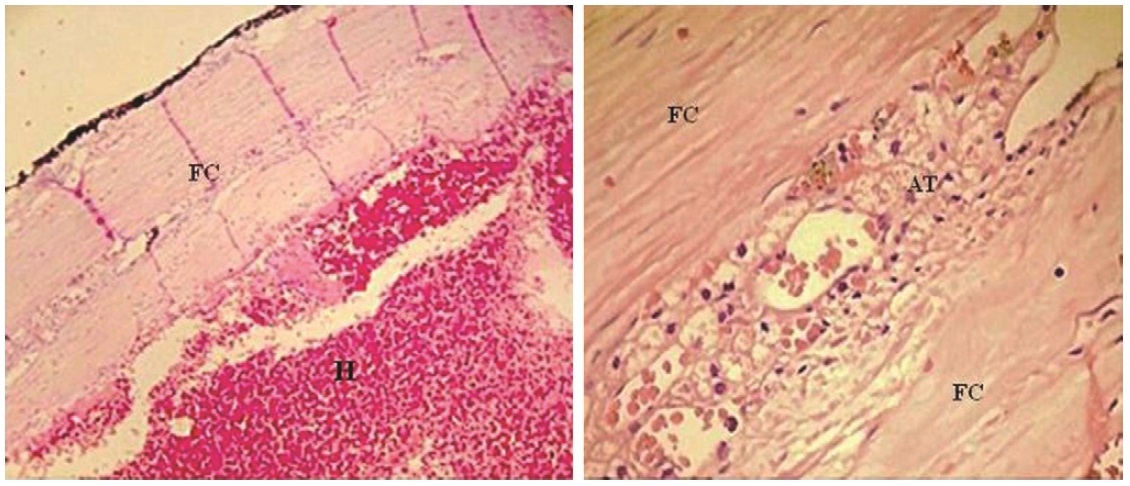
Click here to download Figure 4Figure 4. On low magnification [H&E, x 100] (left) the mass shows mostly diffuse hemorrhage (H) capped by a thin fibrous capsule (FC). On higher magnification [H&E, x 400] (right), benign adrenal tissue (AT) is seen compressed within the fibrous capsule with microhemorrhages within the parenchyma.
Adrenal hemorrhage is an uncommon condition that is of serious concern as it may result in life threatening adrenal insufficiency and even death. It may be caused by several factors including infection, MI, CHF, anticoagulants, trauma, surgery, and antiphospholipid syndrome. None of these conditions were present in our patient. In most of the reported case it is an autopsy finding and the underlying disease mechanism has not been fully elucidated. The adrenal gland is highly vascular and vulnerable to hemorrhage by nature. Small adrenal branches from the three main adrenal arteries form a subcapsular plexus, and the gland is drained by relatively few venules. The term "adrenal dam" has been ascribed to vascularities within the adrenals, implying the large degree of adrenal vascularities that are susceptible to hemorrhage due to their distinct anatomical attributes. While some have suggested that reduced capillary resistance as a result of aging may be a factor, others have postulated that elevated catecholamines and ACTH as a result of stress increases adrenal vascularity and increases adrenal venous pressure due to vasoconstriction, resulting in intraglandular hemorrhage.5-7
Adrenal masses, when discovered, must be further worked up to determine its nature, whether they may be hormonally active or nonfunctional and malignant or benign. A report by Young included 2005 patients in whom adrenal incidentalomas were detected, adrenocortical carcinoma was found in 4.7% of the patients and metastatic cancer in 2.5%. The size of the mass and its appearance on imaging are the two major predictors of malignant disease.8,9 Measurement of precontrast Hounsfield units (HU) and contrast washout on computed tomography scan provide useful diagnostic information.10 Noncontrast CT attenuation coefficient expressed in Hounsfield units (HU) has been increasingly used to differentiate adrenal adenomas from nonadenomas. This is based on the fact that intracytoplasmic fat is often abundant in adrenal adenomas but rare in adrenal metastases, pheochromocytomas, or adrenocortical carcinomas. Threshold values for noncontrast CT HU ranging from 0-20 have been suggested and a 10-HU cutoff value for benign lesions was recommended by a consensus panel organized by the National Institutes of Health.11 The size of the mass of this patient at 14 cm with compression of its adjacent structures as well as characteristics on CT scan that were indicative of malignancy including a Hounsfield unit (HU) ranging between 15 and 40, was an indication for surgery. Hormonal work-up to determine the malignant potential of the tumor was done including screening for glucocorticoid excess, sexual hormones and steroid precursors, mineralocorticoid excess, as well as the exclusion of pheochromocytoma.12 Results revealed a non functional tumor.
Majority of the patients with adrenal bleeding do not show any signs of adrenal insufficiency. The most common symptoms are hypotension, confusion, lethargy, nausea, vomiting, tachycardia, and fever. More specific symptoms such as central abdominal pain radiating to the flank are experienced by 45% of the patients. These symptoms together with anticoagulation therapy in an elderly or very young patient should raise clinical suspicion. In these cases, CT is an essential diagnostic tool.1 On CT scan adrenal hemorrhage appears heterogeneous rather than homogeneous with or without calcification and has a variable density. Adrenal hematomas are usually of soft tissue density but they can also be hypo-attenuated centrally with a peripheral rim of higher attenuation, hyper-attenuated centrally with a rim of hypodensity or hyper-dense. The only specific sign of hematoma, especially with acute hemorrhage, is a spontaneous homogeneous density greater than 50 Hounsfield units. Idiopathic unilateral adrenal hematoma, when diagnosed at a subacute or chronic stage, cannot be distinguished clearly from other lesions on the basis of morphology or density on CT. Findings of a mass with no enhancement or enhancement only in the pattern of a thin peripheral rim agree with the findings of others. This criterion can be valuable in differentiating hematoma from other tumors, with carcinoma and pheochromocytoma almost always have pronounced enhancement.2
An MRI is the ideal imaging modality in studying the adrenal mass in that it may determine the age of the hematoma. In the acute stages, the hematoma typically appears isointense on T1-weighted images and markedly hypointense on T2-weighted images, while in the chronic stages a hypointense rim is present in T1 and T2 weighted images.4
Adrenal hemorrhage is an uncommon condition and is difficult to diagnose because of its nonspecific presentation that the diagnosis is often made at autopsy.8 The value of imaging modalities with the use of CT scan or MRI allows one to determine certain characteristics of an adrenal mass that can point to a benign or malignant tumor. The size and characteristics of the adrenal mass of this patient on CT scan indicated a possibility of malignancy. Further hormonal work-up was warranted and only on post surgical histopathology was the diagnosis of adrenal hemorrhage made. This patient, with no known predisposing factors for bleeding, with no history of intake of anti-coagulant nor history of trauma suffered from an idiopathic adrenal hemorrhage without any hormonal disturbances.
An accurate diagnosis of idiopathic adrenal hemorrhage is quite difficult to make prior to surgery. Some imaging modalities are useful in generating a differential diagnosis, but if the potential for malignancy is not excluded, a thorough hormonal work-up is warranted and surgical resection should be taken into consideration.
Dr. Adriano Dela Paz from The Section of Cardiology, Department of Medicine, The Medical City, for sharing this case with us.
1. Imachi H, Murao K, Yoshimoto T, et al. Idiopathic unilateral adrenal hemorrhage in an elderly patient. Endocr. 2010; 37(2):249-52. http://dx.doi.org/10.1007/s12020-010-9310-z.
2. Hoeffel C, Legmann P, Luton JP, Chapuis Y, Fayet-Bonnin P. Spontaneous unilateral adrenal hemorrhage: Computerized tomography and magnetic resonance imaging findings in 8 cases. J Urol. 1995;154(5):1647-51. 3. Vella A, Nippoldt TB, Morris JC III. Adrenal hemorrhage: A 25-year experience at the Mayo Clinic. Mayo Clin Proc. 2001; 76(2):161-8. http://dx.doi.org/10.4065/76.2.161. 4. Kawashima A, Sandler CM, Ernst RD, et al. Imaging of nontraumatic hemorrhage of the adrenal gland. Radiographics. 1999;19(4): 949-63. 5. Dhawan N, Bodukam VK, Thakur K, Singh A, Jenkins D, Bahl J. Idiopathic Bilateral Adrenal Hemorrhage in a 63-year-old male: A case report and review of the literature. Case Rep Urol. 2015;2015. http://dx.doi.org/10.1155/2015/503638. 6. Sasaki K, Yamada T, Gotoh K, et al. Idiopathic adrenal hematoma masquerading as neoplasm. Case Rep Gastroenterol. 2012 Jan;6(1):171-6. 7. Christoforides C, Petrou A, Loizou M. Idiopathic unilateral adrenal haemorrhage and adrenal mass: A case report and review of the literature. Case Rep Surg. 2013;2013. http://dx.doi.org/10.1155/ 2013/567186. 8. Young WF Jr. Management approaches to adrenal incidentalomas: a view from Rochester, Minnesota. Endocrinol Metab Clin North Am. 2000;29:159-185. 9. Young WF Jr. The incidentally discovered adrenal mass. N Engl J Med. 2007;356:601-610. http://dx.doi.org/10.1056/NEJMcp065470. 10. Nieman L. Approach to the patient with an adrenal incidentaloma. J Clin Endocrinol Metab. September 2010; 95(9):4106-4113. http://dx.doi.org/10.1210/jc.2010-0457. 11. Hamrahian A, Ioachimescu AG, Remer EM, et al. Clinical utility of noncontrast computed tomography attenuation value (Hounsfield Units) to differentiate adrenal adenomas/hyperplasias from nonadenomas: Cleveland clinic experience. J Clin Endocrinol Metab. 2005;90(2):871-77. http://dx.doi.org/10.1210/jc.2004-1627. 12. Allolio B, Fassnacht M. Clinical review: Adrenocortical carcinoma: Clinical update. J Clin Endocrinol Metab. 2006;91(6):2027-2037. htpp://dx.doi.org/10.1210/jc.2005-2639.Authors are required to accomplish, sign and submit scanned copies of the JAFES Declaration that the article represents original material that is not being considered for publication or has not been published or accepted for publication elsewhere.
Consent forms, as appropriate, have been secured for the publication of information about patients; otherwise, authors declared that all means have been exhausted for securing such consent.
The authors have signed disclosures that there are no financial or other relationships that might lead to a conflict of interest. All authors are required to submit Authorship Certifications that the manuscript has been read and approved by all authors, and that the requirements for authorship have been met by each author.