Accurate assessment of adrenocortical function is essential in the management of patients with suspected adrenal insufficiency (AI). If left untreated, adrenal crisis with features of severe vomiting, shock, confusion, loss of consciousness or even death might result during acute stress. The low dose 1 μg short Synacthen® test (LDSST) is considered to be the gold standard to evaluate adrenal function in such patients. A maximum cortisol response between 400 to 620 nmol/L within 20 to 40 minutes after intravenous administration of 1 &um;g of synthetic adrenocorticotropin (ACTH) (Synacthen®) are variably used for the diagnosis of adrenal sufficiency.1-6
In patients with recent onset ACTH deficiency (e.g. within 2 weeks after pituitary surgery), the adrenal glands may not have become completely atrophic and may still respond to ACTH stimulation.1,2 For this reason, the insulin tolerance test (ITT) is traditionally seen as the gold standard for investigation of the integrity of the hypothalamic-pituitary-adrenal (HPA) axis in secondary adrenal insufficiency. However, the ITT carries a risk of hypoglycemia, and is contraindicated for patients with epilepsy, ischemic heart disease or recent cerebrovascular accident.3 The metyrapone test may also be used in evaluating the HPA axis. Its use is limited because metyrapone may precipitate refractory hypotension in some patients, and the measurement of 11-deoxycorticosterone is not readily available in most laboratories.4,5 Other stimulation tests, such as the glucagon or the corticotropin-releasing hormone tests, are not as sensitive and specific as ITT.6,7 The LDSST has been validated as a safe and sensitive method for screening abnormalities of the HPA axis in Chinese patients suspected of having secondary adrenocortical insufficiency.8 Earlier studies indicate that LDSST can also detect partial adrenal insufficiency, such as in cases of chronic use of inhaled glucocorticoids or early adrenal destruction by infectious or autoimmune processes. These may be missed by the standard dose short Synacthen® test (SST), which involves a supraphysiologic stimulus that can stimulate a compromised adrenal gland that still has some residual function.9,10 In our hospital, a peak cortisol response in LDSST at or above 500 nmol/L is accepted as adequate adrenal reserve in a patient with suspected adrenal insufficiency (primary, or secondary if at least 2 weeks post pituitary surgery).
The LDSST procedure involves intravenous administration of Synacthen® and venous blood sample collection at 0, 20 and 30 minutes for measurement of serum cortisol. In our center, cortisol is measured by electrochemiluminescence immunoassay (Roche Diagnostics, Basel, Switzerland). The test is labor intensive, invasive and inconvenient. The requirement of multiple blood sampling is poorly accepted by patients, especially those who are subjected to the test on a regular basis. A simpler test, such as a spot or morning cortisol, has been evaluated to indicate cortisol reserve.11,12 In the Caucasian population, a 9 am serum cortisol of <100 nmol/L or >500 nmol/L has been validated as adrenal insufficient or adrenal sufficient, respectively, eliminating the need for further complicated stimulation tests.13 It was observed that the number of LDSST yielding results consistent with normal adrenal reserve (85%, unpublished data) was more than expected in our hospital as compared to a previous studies (69% to 71%).13,14 This prompted the question as to whether too many patients were put through unnecessary invasive procedures, and whether this could be reduced by measuring spot or morning serum cortisol prior to the stimulation test.
The aims of this study were:
1. To assess the usefulness of spot serum cortisol in the diagnosis of patients with suspected primary or secondary adrenocortical insufficiency, using LDSST as the gold standard diagnostic test, and to identify the optimal cut-off values for spot cortisol in the Chinese population in the in-patient setting; and
2. To assess the usefulness of morning serum cortisol in the diagnosis of patients with suspected primary or secondary adrenocortical insufficiency, using LDSST as the gold standard diagnostic test, and to identify the optimal cut-off values for morning cortisol in the Chinese population in the out-patient setting.
The study was carried out in two phases at the Prince of Wales Hospital, the teaching hospital of the Chinese University of Hong Kong. The first phase was a retrospective analysis of data from 423 in-patients included consecutively from July 2013 to December 2013. All patients were evaluated with LDSST because of suspected disease of the HPA axis for various reasons, such as hyponatremia, hypotension, hypoglycemia or suspected iatrogenic Cushing's syndrome, during their hospitalization for acute illnesses. The LDSST was performed by a house officer at any time of the day, usually within 12 hours from the time the order was placed by a medical officer. One mL (0.25 mg) of Synacthen® was added to 499 mL of normal saline. After mixing thoroughly, 2 mL of the freshly mixed solution (containing 1 μg Synacthen®) was withdrawn into a syringe. Blood was drawn for 0 minute serum cortisol, followed by an intravenous bolus injection of Synacthen® 1 μg. Blood was again sampled for cortisol measurement at 20 and 30 minutes after the injection. Serum cortisol levels were assayed at each time point by electrochemiluminescence immunoassay (Roche Diagnostics, Basel, Switzerland). The lower limit for detection was assessed to be 0.5 nmol/L. The coefficient of variation at different levels for the assay were 3.8% at 104 nmol/L, 2.5% at 700 nmol/L and 2.6% at 1045 nmol/L.
The second phase was a prospective analysis of 422 out-patients recruited consecutively from June 2014 to October 2014. All patients were evaluated with LDSST because of suspected disease of the HPA axis when free from acute stress. The patients were categorized into 4 groups based on the reasons for referral:
Category 1: Patients referred from in-patient at discharge, excluding those in categories 2 and 3;
Category 2: Patients with pituitary lesion or disturbance;
Category 3: Patients who were on exogenous steroid or had adrenalectomy done due to adrenal Cushing's syndrome; and
Category 4: Patients referred for reasons not included in the previous 3 categories.
The LDSST was carried out in the out-patient Endocrine Centre by a specialty nurse at 0900H. The steps of the test and the cortisol assay were exactly the same as those in the first phase of the study.
Receiver operating characteristic (ROC) curves were obtained using the Statistical Package for Social Sciences version 21 (SPSS Inc., Chicago, Illinois).
Phase One (In-patients, retrospective)
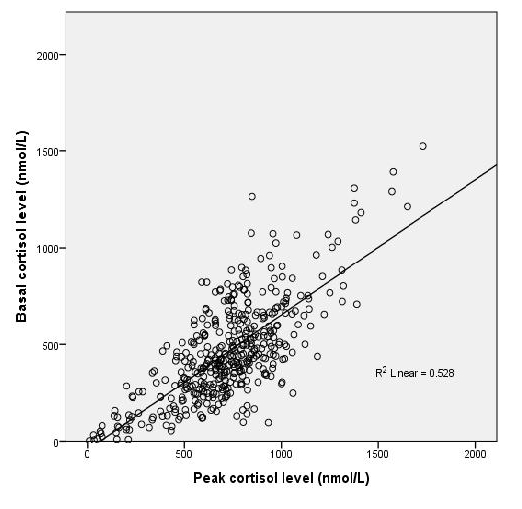
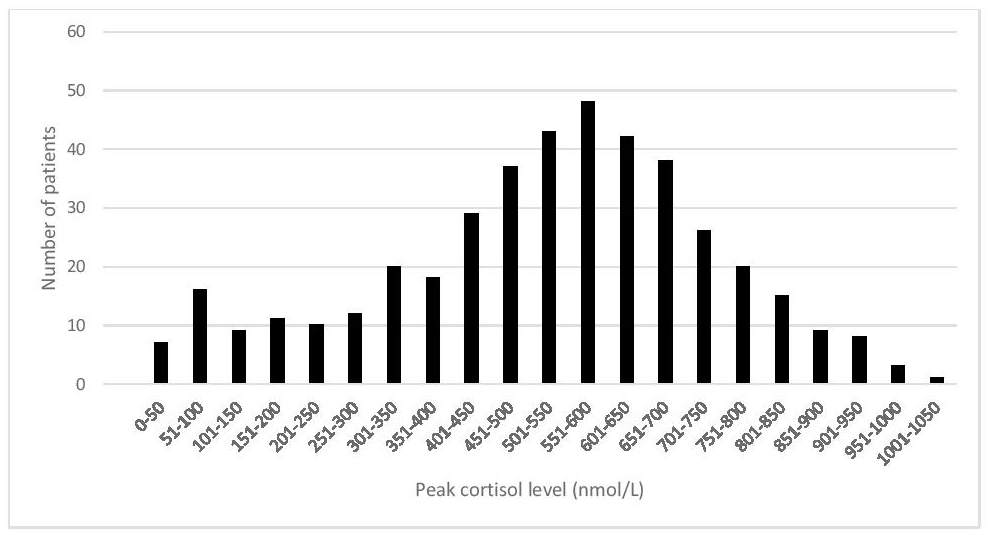
423 in-patients with suspected adrenal insufficiency underwent LDSST during their hospitalization for acute illnesses over a 6-month period. Only a small proportion, 15%, failed the LDSST. Both basal and peak cortisol ranges were lower in patients who failed the test (Table 1). The peak cortisol of these patients were normally distributed (Appendix 1). There was a significant correlation between basal cortisol values and peak levels during the LDSST (R2=0.528) (Figure 1). ROC analysis suggested the safest baseline cortisol cut-off point of ≤92 nmol/L as an indication of adrenal insufficiency, resulting in 100% sensitivity and 32% specificity. A cortisol cut-off point of ≥494 nmol/L was found have 100% specificity, but with only 45% sensitivity (Figure 2). Twenty (4.7%) patients had basal cortisol =92 nmol/L, while 163 (38.5%) had values ≥494 nmol/L.
Click here to download Table 1Table 1. Cortisol levels of im-patients with low dose short Synacthen® test performed over a 6-month period (N=423)

Click here to download Appendix 1
Appendix 1. Peak cortisol levels in low dose short synacthen tests in 423 in-patients.

Click here to download Figure 1
Figure 1.Individual cortisol peak levels in 423 in-patients plotted against basal cortisol during low dose short Synacthen® test.
Click here to download Figure 2
Figure 2. Receiver operating characteristic curve of basal cortisol levels in 423 in-patients with the low dose short Synacthen® test (LDSST) as reference test. Peak cortisol levels in the LDSST less than 500 nmol/L indicate adrenal insufficiency. Area under the curve 0.884 (95% confidence intervals 0.852-0.917).

Phase Two (Out-patients, prospective)
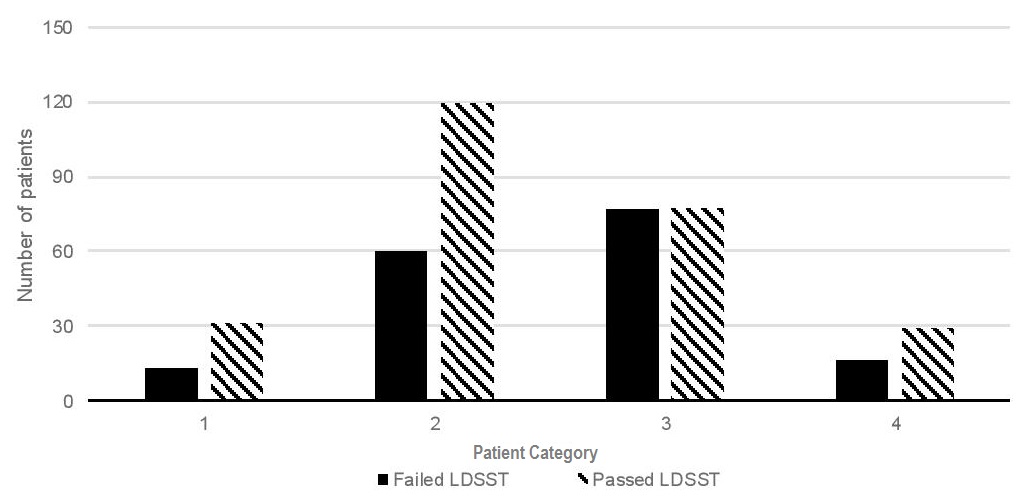
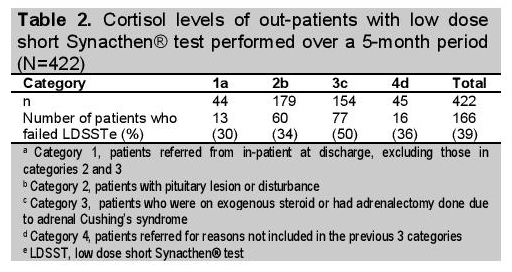
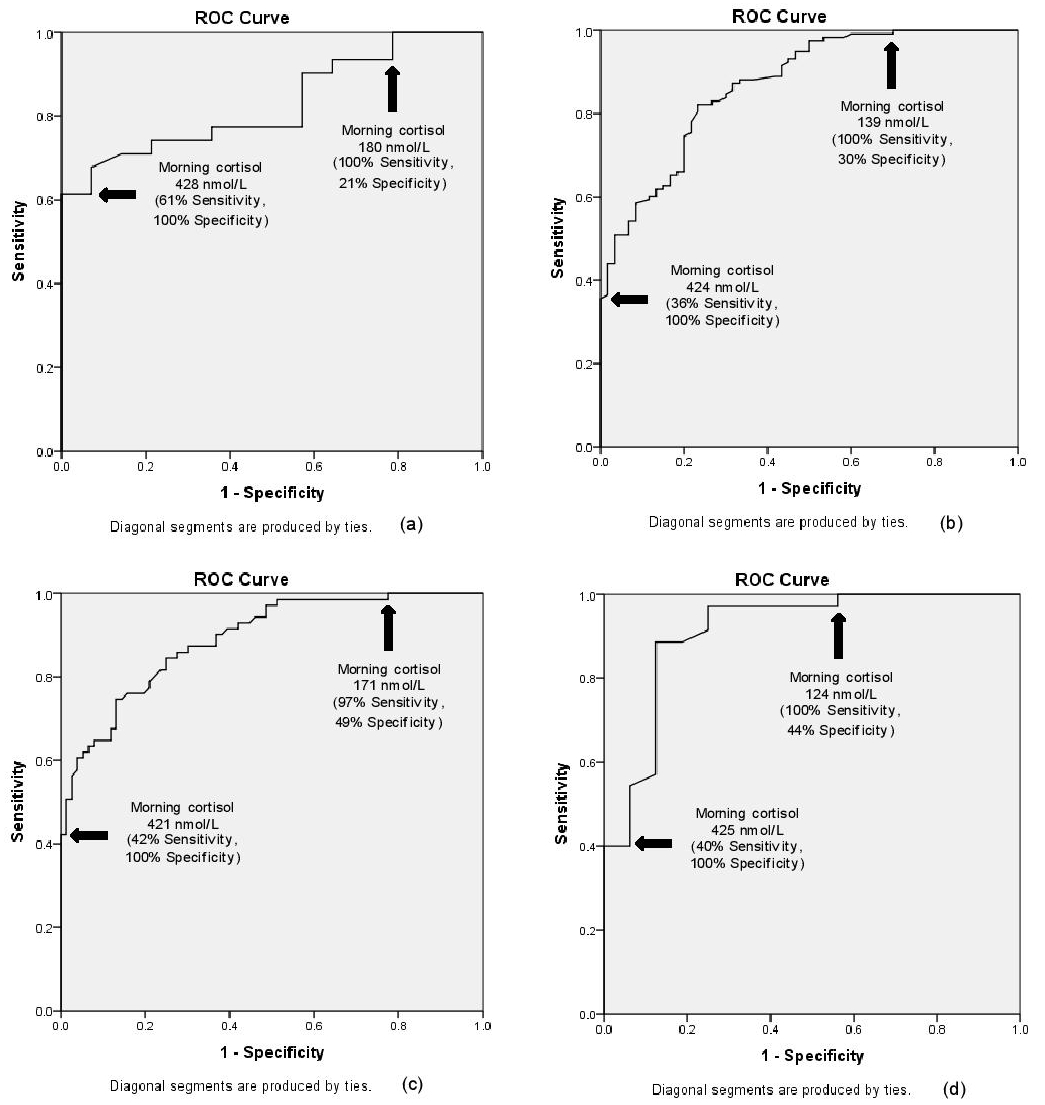
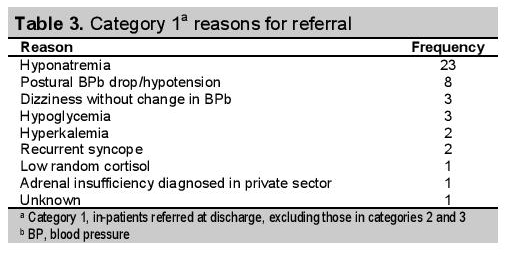
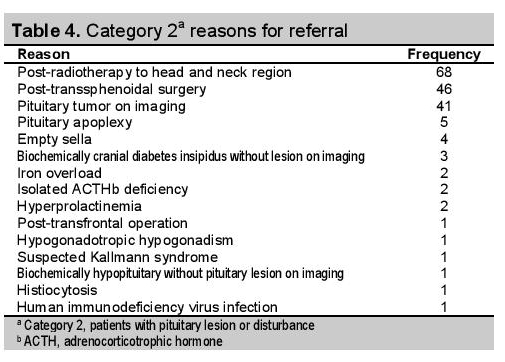
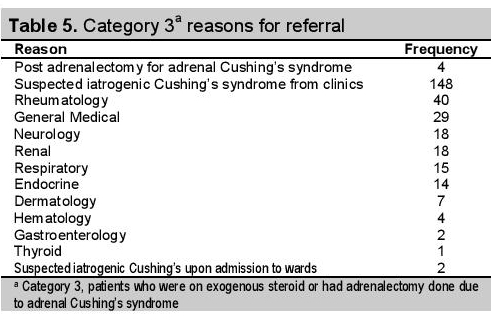
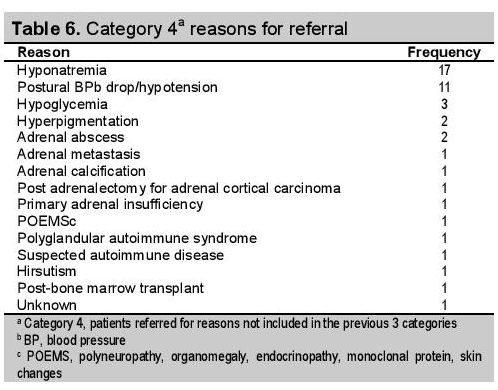
422 out-patients with suspected adrenal insufficiency underwent LDSST in the out-patient Endocrine Centre when they were not under acute stress over a 5-month period. The peak cortisol of these patients were normally distributed (Appendix 2). The number of patients in each out-patient category stratified by their responses to the LDSST is illustrated in Figure 3. Fifty percent of the patients in category 3 failed the LDSST. The proportion of patients who failed the LDSST were similar across category 1, 2, and 4 (30 to 36%). A summary of the responses and reasons for referral for LDSST is presented in Table 2. Most patients were category 2, with radiotherapy to the head and neck region as the most common reason for referral. For both categories 1 and 4, hyponatremia was the most frequently cited reason for referral, followed by postural BP drop or hypotension. Suspicion of iatrogenic Cushing's syndrome made up the majority of referrals in category 3 (150 out of 154 patients), most frequently referred from Rheumatology, followed by general medical clinics. Two patients had no clear reasons for referral despite detailed review of their medical records: one in category 1 (referred from in-patient) and one in category 4 (referred from out-patient). A vast variety of reasons for referral were noted in category 4, ranging from abnormal biochemistry results (hyponatremia or hypoglycemia), general signs or symptoms (postural BP drop/hypotension or hyperpigmentation), localized adrenal abnormalities (adrenal abscess, metastasis, calcification, or resection), to endocrine syndromes [polyneuropathy, organomegaly, endocrinopathy, monoclonal protein and skin changes (POEMS); or polyglandular autoimmune syndrome (PAS)]. ROC curves for patients in different categories showed that the safest morning cortisol cut-offs as signals of adrenal insufficiency or sufficiency in the out-patient population were different for patients in different categories (Figure 4). Taken as a whole, the most sensitive serum cortisol level indicative of adrenal insufficiency was ≤124 nmol/L, the lowest cut-off across all categories with a sensitivity of 100%. A serum cortisol of ≥428 nmol/L, the highest cut-off across all categories with a 100% specificity, was the most specific level that ruled out adrenal insufficiency. Fifty-three patients (12.6%) had morning cortisol levels =124 nmol/L, while 101 (23.9%) had levels ≥428 nmol/L.
Click here to download Appendix 2Appendix 2. Peak cortisol levels in low dose short synacthen tests in 422 out-patients.
Click here to download Figure 3
Figure 3.Number of patients in each out-patient category stratified by their responses to low dose short Synacthen® test. Category 1: Patients referred from in-patient at discharge, excluding those in categories 2 and 3; Category 2: Patients with pituitary lesion/disturbance; Category 3: Patients who were on exogenous steroid or had adrenalectomy done due to adrenal Cushing's syndrome; Category 4: Patients referred for other reasons.
Click here to download Table 2
Table 2. Cortisol levels of out-patients with low dose short Synathen® test performed over a 5-month period (N=422)
Click here to download Figure 4
Figure 4.Receiver operating characteristic curves of morning cortisol levels in 422 out-patients with the low dose short Synacthen® test (LDSST) as reference test. Peak cortisol levels in the LDSST less than 500 nmol/L indicate adrenal insufficiency. (a) Category 1: In-patients reffered upon discharge, excluding those in categories 2 and 3; area under the curve (AUC) 0.828 (95% confidence intervals 0.711-0.945). (b) Category 2: Patients with pituitary lesion/disturbance; AUC 0.869 (95% confidence intervals 0.817-0.922). (c) Category 3: Patients who were on exogenous steroid or had adrenalectomy done due to adrenal Cushing's syndrome; AUC 0.879 (95% confidence intervals 0.824-0.933). (d) Category 4: Patients referred for other reasons; AUC 0.913 (95% confidence intervals 0.820-1.000).
Click here to download Table 3
Table 3.Category 1a reasons for referral
here to download Table 4
Table 4. Category 2a reasons for referral)
here to download Table 5
Table 5.Category 3a reasons for referral
here to download Table 6
Table 6.Category 4a reasons for referral
Discussion
Simpler and non-invasive tests to diagnose adrenal insufficiency, such as spot or morning serum cortisol, could possibly reduce the number of patients having to go through the cumbersome LDSST. In this study, we compared basal cortisol levels with LDSST in a group of in-patients, to determine their utility in being the first step screening test for evaluation of AI. We also compared the morning cortisol levels with the LDSST in a group of out-patients referred for suspected AI, and determined the safest cut-offs for identification of patients requiring further dynamic tests. The disease spectrum leading to suspicion of AI in our Chinese out-patient cohort is described in Table 2.
Roux studied a cohort of 210 patients with suspected AI to determine the utility of the 9 AM cortisol level prior to SST in out-patient assessment using automated enzyme-linked immunosorbent assay (ELISA) with the Roche Diagnostics ES700 (Lewes, UK). The study found that the SST is of little added value in patients with a 9 AM cortisol of <100 nmol/L or >500 nmol/L. They recommended a 9 AM cortisol level should be included in the appropriate protocols for endocrine workup, since it would have prevented 21% of the patients from going through unnecessary SST.13 Our investigation of 422 Chinese out-patients revealed similar values: patients with morning cortisol levels ≤124 nmol/L (n=53) and ≥428 nmol/L (n=101) were all adrenal insufficient and adrenal sufficient, respectively. Therefore, further LDSST for these groups of patients (37% of the original 422 patients) would not have been indicated. Similarly, for our in-patient cohort, 43% of the original 423 patients would not have needed the LDSST based on the spot cortisol cut-offs of ≤92 nmol/L (adrenal insufficient) and ≥494 nmol/L (adrenal sufficient). Our higher percentage of unnecessary dynamic test as compared to Roux's study may be the result of a lower clinical threshold for referral in our Centre. However, since the exact reasons for referral were not specified in Roux's paper, we are unable to further examine this hypothesis.
In our study, the cortisol cut-off level for the diagnosis of adrenal insufficiency with the best sensitivity and specificity was lower for in-patients (92 nmol/L) than out-patients (124 nmol/L). The percentage of unnecessary LDSST was higher in the in-patient cohort (43%) than the out-patient cohort (37%). Because the in-patients were under acute stress and the out-patients were ambulatory and not acutely ill, the cortisol levels in these groups cannot be directly compared. The clinical threshold of suspecting adrenal insufficiency is also lower for in-patients, since they are often very ill, leading to a higher number of unnecessary LDSST.
Fifteen percent of the in-patients failed the LDSST. For the out-patients, the percentage of patients failing the LDSST were similar for categories 1, 2 and 4 (30 to 36%). Remarkably, 50% of those in category 3 failed the LDSST. Chronic adrenal suppression, either by exogenous steroid or excessive endogenous steroid from a functioning adrenal adenoma, made them more prone to genuine adrenal insufficiency.
Cushing's syndrome due to exogenous steroid is common, as about 1% of the general population use exogenous steroids for various indications.15 A recent study from the United Kingdom reported that up to 33.2% of patients on exogenous steroids had a subnormal response to short Synacthen® test when cortisol levels were analyzed with a standard automated competitive immunoassay platform (Roche 114 Modular System, Roche, Lewes, UK).16 Nasopharyngeal carcinoma (NPC) is a major public health concern in Hong Kong with an annual incidence of 15.4 in 100,000, with radiotherapy being the most commonly used modality of treatment since decades ago.17 Therefore, it is not surprising that these two groups of patients made up the majority of our out-patient cohort (52%). Both groups are often regularly tested for adrenal function to monitor adrenal recovery in iatrogenic Cushing's and adrenal failure in NPC. Currently, these patients are all being managed by internal medicine specialists in our hospital, taking up a significant share of consults in the internal medicine clinics. Informing the family doctors about the morning cortisol range needing LDSST derived from this study (124 to 428 nmol/L) would help them make rational decisions on who would need follow-up LDSST to diagnose AI, and who would have to be referred to internal medicine clinics when LDSST is needed. This huge number of patients may be managed adequately in the family medicine clinics, while more clinic quota in the internal medicine clinics may be spared for other patients in need.
In should be emphasized that a normal spot/morning cortisol or even LDSST result does not preclude the use of glucocorticoid stress coverage if the clinical picture is strongly suggestive of adrenal insufficiency, especially during extreme physiological stress. While adrenal sufficiency was defined as an adequate serum cortisol response of >500 nmol/L at either 20 or 30 minutes after intravenous Synacthen® for the purpose of this study, this assumption may not always be applicable in clinical practice. LDSST cut-offs were obtained from either 2.5th or 5th percentile values from testing normal individuals, implying an intrinsic error rate when using this test.18 Physicians ordering spot/morning cortisol or LDSST should always interpret the results within the specific clinical context when making a diagnosis of adrenal insufficiency.
Our study has several limitations. First, the timing of LDSST for in-patients was not standardized. Due to practicability issues within our stretched health-care system, our house officers could only attend to dynamic function tests after completion of all on-hand urgent duties, making it difficult to have tests done at 0900H. As cortisol secretion follows a diurnal rhythm, this lack of standardization might impair the applicability of our analyses. Nevertheless, acute stress is known to affect diurnal rhythm, so that standardizing the timing of LDSST at 0900H for in-patients may not be as important as those performed in out-patients who do not have acute illnesses.19 Second, concomitant blood glucose levels during cortisol measurements that may influence cortisol responses in acutely ill patients were not accounted for since the data were not captured. Third, since 80% of plasma cortisol is bound by cortisol-binding globulin (CBG), and that many conditions (thyrotoxicosis, hypothyroidism, chronic liver disease, nephrotic syndrome, use of oral contraceptive pills) may affect the levels of CBG and levels of free cortisol, the measurements of CBG with serum cortisol would have improved the accuracy of our analyses.20-22 Fourth, for patients with suspected secondary adrenal insufficiency due to exogenous glucocorticoids, information on the dose, route, potency and duration were not available for assessment of dose-dependent effects. However, the expectation would be intuitive, so that the larger dose, longer duration, more potent the glucocorticoids used, the more likely that secondary adrenal insufficiency would result. Fifth, the duration of pituitary disease was not captured in this study. Sixth, as this is a continual quality improvement project in our hospital, instead of a defined sample size, a designated time period was followed according to the project timeline set by the hospital management team. Lastly, since it has been shown that different assays yield different cortisol cut-offs for confirmation of AI, results and interpretations from our study cannot be directly compared with those from studies using different assays.23
Despite these limitations, the clear separation of patients into those with acute illnesses (in-patients) and those without acute stress (out-patients), the relatively large sample size for both the in- and out-patients cohorts, and the detailed categorization of the out-patient cohort are important strengths of this study.
We found that he LDSST is of little added value in in-patients with spot serum cortisol of ≤92 nmol/L or ≥494 nmol/L, and out-patients with morning serum cortisol of =124 nmol/L or ≥428 nmol/L. Spot and morning cortisol levels, for in- and out-patients respectively, should be incorporated into endocrine protocols preceding the LDSST in the workup of adrenal insufficiency in order to free up manpower, reduce waiting time in specialists' clinics, and to save patients from unnecessary invasive investigations.
Acknowledgements
We thank Michael Chan and Jeffrey Kwok for their support in performing cortisol assays in the Department of Chemical Pathology, The Chinese University of Hong Kong, Prince of Wales Hospital, New Territories, Hong Kong.
Address all correspondence and requests for reprints to: Kitty Kit-Ting Cheung, MRCP, FHKCP, FHKAM (Medicine), Department of Medicine and Therapeutics, The Chinese University of Hong Kong, Prince of Wales Hospital, New Territories, Hong Kong.
Disclosure Summary: The authors declare the absence of any conflict of interest that could be perceived as prejudicing the impartiality of the research reported.
1. Cunningham SK, Moore A, McKenna TJ. Normal cortisol response to corticotropin in patients with secondary adrenal failure. Arch Intern Med. 1983;143(12):2276-9.
2. Lindholm J, Kehlet H. Re-evaluation of the clinical value of the 30 min ACTH test in assessing the hypothalamic-pituitary-adrenocortical function. Clin Endocrinol (Oxf). 1987;26(1):53-9. http://dx.doi.org/10.1111/j.1365-2265.1987.tb03638.x. 3. Fish HR, Chernow B, O'Brian JT. Endocrine and neurophysiologic responses of the pituitary to insulin-induced hypoglycemia: A review. Metabolism.1986;35(8):763-80. 4. Fiad TM, Kirby JM, Cunningham SK, McKenna TJ. The overnight single-dose metyrapone test is a simple and reliable index of the hypothalamic-pituitary-adrenal axis. Clin Endocrinol (Oxf). 1994;40(5):603-9. http://dx.doi.org/10.1111/j.1365-2265.1994.tb03011.x. 5. Grinspoon SK, Biller BM. Clinical review 62: Laboratory assessment of adrenal insufficiency. J Clin Endocrinol Metab. 1994;79(4):923-31. http://dx.doi.org/10.1210/jcem.79.4.7962298. 6. Orme SM, Peacey SR, Barth JH, Belchetz PE. Comparison of tests of stress-released cortisol secretion in pituitary disease. Clin Endocrinol (Oxf). 1996;45(2):135-40. http://dx.doi.org/10.1046/j.1365-1996.d01-1562.x. 7. Schulte HM, Chrousos GP, Avgerinos P et al. The corticotropin-releasing hormone stimulation test: a possible aid in the evaluation of patients with adrenal insufficiency. J Clin Endocrinol Metab. 1984;58(6):1064-7. http://dx.doi.org/10.1210/jcem-58-6-1064. 8. Choi CH, Tiu SC, Shek CC, Choi KL, Chan FK, Kong PS. Use of the low-dose corticotropin stimulation test for the diagnosis of secondary adrenocortical insufficiency. Hong Kong Med J. 2002;8(6):427-34. 9. Streeten DH, Anderson GH Jr, Bonaventura MM. The potential for serious consequences from misinterpreting normal responses to the rapid adrenocorticotropin test. J Clin Endocrinol Metab. 1996;81(1):285-90. http://dx.doi.org/10.1210/jcem.81.18550765. 10. Broide J, Soferman R, Kivity S et al. Low-dose adrenocorticotropin test reveals impaired adrenal function in patients taking inhaled corticosteroids. J Clin Endocrinol Metab. 1995;80(4):1243-6. http://dx.doi.org/10.1210/jcem.80.4.7714095. 11. Hagg E, Asplund K, Lithner F. Value of basal plasma cortisol assays in the assessment of pituitary-adrenal insufficiency. Clin Endocrinol (Oxf). 1987;26(2):221-6. http://dx.doi.org/10.1111/j.1365-2265.1987.tb00780.x. 12. Courtney CH, McAllister AS, McCance DR et al. Comparison of one week 0900 h serum cortisol, low and standard dose synacthen tests with a 4 to 6 week insulin hypoglycaemia test after pituitary surgery in assessing HPA axis. Clin Endocrinol (Oxf). 2000;53(4):431-6. http://dx.doi.org/10.1046/j.1365-2265.2000.01106.x. 13. Le Roux CW, Meeran K, Alaghband-Zadeh J. Is a 0900-h serum cortisol useful prior to a short synacthen test in outpatient assessment? Ann Clin Biochem. 2002;39(Pt 2):148-50. http://dx.doi.org/10.1258/0004563021901919. 14. Yo WS, Toh LM, Brown SJ, Howe WD, Henley DE, Lim EM. How good is a morning cortisol in predicting an adequate response to intramuscular synacthen stimulation? Clin Endocrinol (Oxf). 2014;81(1):19-24. http://dx.doi.org/10.1111/cen.12373. 15. Prague JK, May S, Whitelaw BC. Cushing's syndrome. BMJ. 2013;346:f945. http://dx.doi.org/10.1136/bmj.f945. 16. Woods CP, Argese N, Chapman M et al. Adrenal suppression in patients taking inhaled glucocorticoids is highly prevalent and management can be guided by morning cortisol. Eur J Endocrinol. 2015;173(5):633-42. http://dx.doi.org/10.1530/EJE-15-0608. 17. Lee AW, Ng WT, Chan LL et al. Evolution of treatment for nasopharyngeal cancer--success and setback in the intensity-modulated radiotherapy era. Radiother Oncol. 2014;110(3):377-84. http://dx.doi.org/10.1016/j.radonc.2014.02.003. 17. Lee AW, Ng WT, Chan LL et al. Evolution of treatment for nasopharyngeal cancer--success and setback in the intensity-modulated radiotherapy era. Radiother Oncol. 2014;110(3):377-84. http://dx.doi.org/10.1016/j.radonc.2014.02.003. 18. Clark PM, Neylon I, Raggatt PR, Sheppard MC, Stewart PM. Defining the normal cortisol response to the short Synacthen test: implications for the investigation of hypothalamic-pituitary disorders. Clin Endocrinol. 1998;49(3):287-92. http://dx.doi.org/10.1046/j.1365-2265.1998.00555.x. 19. Hulme PA. A clinical translation of the research article titled "changes in diurnal salivary cortisol levels in response to an acute stressor in healthy young adults". J Am Psychiatr Nurses Assoc. 2011;17(5):350-5. http://dx.doi.org/10.1177/1078390311422564. 20. Wand GS, Ney RL. Disorders of the hypothalamic-pituitary-adrenal axis. Clin Endocrinol Metab.1985;14(1):33-53. 21. Gleeson HK, Walker BR, Seckl JR, Padfield PL. Ten years on: Safety of short synacthen tests in assessing adrenocorticotropin deficiency in clinical practice. J Clin Endocr Metab. 2003;88(5):2106-11. 22. Brien TG. Human corticosteroid binding globulin. Clin Endocrinol (Oxf).1981;14(2):193-212. http://dx.doi.org/10.111/j.1365-2265.1981.tb00616.x. 23. El-Farhan N, Pickett A, Ducroq D et al. Method-specific serum cortisol responses to the adrenocorticotrophin test: comparison of gas chromatography-mass spectrometry and five automated immunoassays. Clin Endocrinol (Oxf). 2013;78(5):673-80. http://dx.doi.org/10.1111/cen.12039.Authors are required to accomplish, sign and submit scanned copies of the JAFES Declaration that the article represents original material that is not being considered for publication or has not been published or accepted for publication elsewhere.
Consent forms, as appropriate, have been secured for the publication of information about patients; otherwise, authors declared that all means have been exhausted for securing such consent.
The authors have signed disclosures that there are no financial or other relationships that might lead to a conflict of interest. All authors are required to submit Authorship Certifications that the manuscript has been read and approved by all authors, and that the requirements for authorship have been met by each author.