Type 1 diabetes mellitus is a common autoimmune disorder of the pediatric population, and it is frequently associated with other autoimmune conditions, especially with autoimmune hypothyroidism and celiac disease.1 Celiac disease, or gluten-sensitive enteropathy, is an autoimmune disorder characterized by inflammation, villous atrophy and crypt hyperplasia of the small bowel mucosa after ingestion of dietary gluten and recovers when gluten-containing cereals are withdrawn from the diet.
The prevalence of rate of celiac disease in type 1 diabetes patients varies from study to study but ranges from 1% to 11%,2 almost 10-20 times higher than that observed in the general pediatric population.3 It has an incidence of 1 in 96 in north India.4
The presentation of celiac disease in Type 1 diabetes patients is extremely variable, with about less than one third of patients presenting with gastrointestinal complaints, some patients remain asymptomatic and are diagnosed during routine screening procedures.5 The prominent extra intestinal manifestations of celiac disease are short stature, delayed puberty, poor glycemic control, nutritional anaemia, etc.6,7
Patients with celiac disease frequently present with growth failure and malnutrition besides hypocalcaemia and anaemia. Suboptimal growth velocity, poor weight gain and glycemic control appears to be multifactorial. Few studies support the role of RANKL/ OPG system in the pathogenesis, but the exact cause for it is still unknown.8
There are very few studies which show the effect of gluten free diet on weight, height, height velocity, and other biochemical parameters in celiac type 1 diabetes patients. There is very limited data from the Indian subcontinent.
The main aim of the present prospective observational study is to study the impact of a gluten-free diet on several growth parameters in children with Type 1 diabetes mellitus and celiac disease in Western Uttar Pradesh, India.
This is a prospective cohort study carried out in the Department of Endocrinology and Metabolism during the study period of 2 years from July 2011 to June 2013.
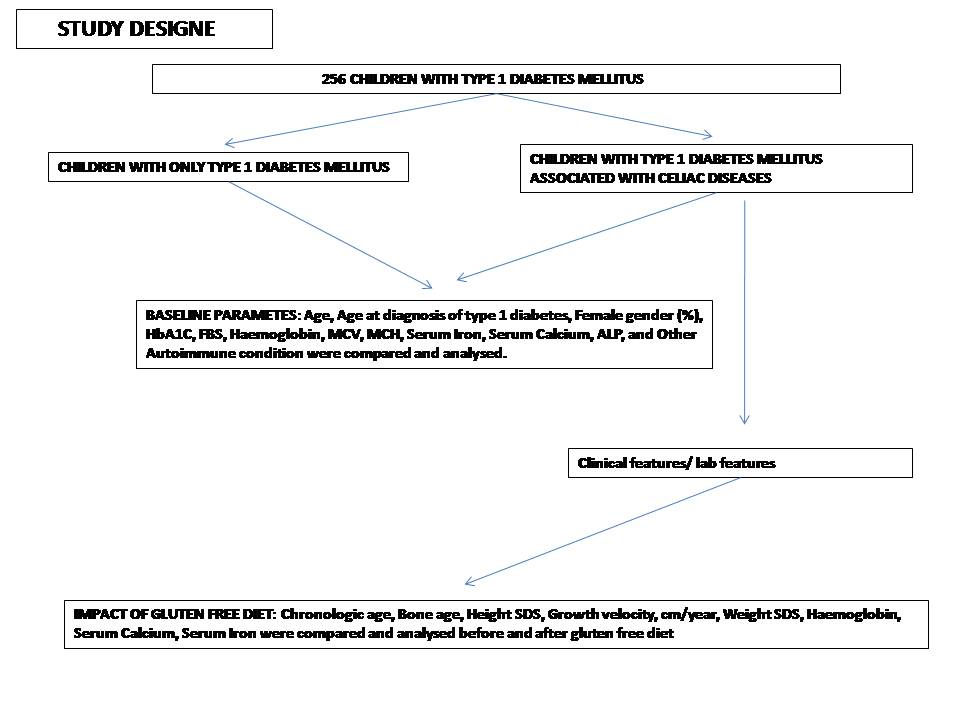
Two hundred and fifty six children and adolescents with type 1 diabetes mellitus, aged 6 to 18 years, presenting to the endocrine OPD or admitted to the endocrinology ward were enrolled in the study (Figure 1). The study was approved by our local ethics committee.
Click here to download Figure 1Figure 1. Study design.
After explaining the objectives of the study, a written informed consent was obtained from the patients or their parents. Patients were evaluated during the study period of two years from July 2011 to June 2013; inquiries were made for family history of other common autoimmune disorders, which are associated with type 1 diabetes.
Physical examination along with anthropometry and Tanner scoring was done by two endocrinologists, including one pediatric endocrinologist.
Blood samples were collected for: anti-TTG immunoglobulin subclass A (IgA) using enzyme linked immunosorbent assay (ELISA), complete blood count (CBC), iron profile, glycosylated hemoglobin (HbA1C), serum calcium, phosphorus and albumin.
Wrist and knee x-rays were done for bone age assessment in all patients with celiac disease in the hospital premises. The x-ray was reported first by experienced endocrinologists and then by radiologists, and if both agreed on a finding, it was accepted. Bone age was assessed using the Tanner Whitehouse 2 (TW2) system.
Short stature is a term used to describe a condition in which a child's or a teen's height is well below the 3rd percentile or 2 standard deviation (SD) below the mean height for age and gender and when the patient's linear growth velocity diminishes to less than 4 cm/yr (child's growth shifts to a lower channel). Delayed bone age was defined as a difference of at least 24 months between chronological age and bone age. Ethical clearance for the study was granted by the institutional ethics committee.
Vitamin D level was requested when deemed appropriate. Endoscopic duodenal biopsies were undertaken in the patients with signs and symptoms suspicious for celiac disease, if they were negative for anti-TTG antibody after informed consent.
Screening for other autoimmune disorders was done only when signs or symptoms were present, or if family history was suggestive of autoimmune disorders.
Statistical AnalysisAll categorical variables were expressed as percentages and all continuous variables were expressed as mean ± standard deviation. Student's t-test for independent samples was used to compare the mean values of continuous study variables. The 95% confidence intervals for difference of mean were used. Chi-square test and Fisher's exact tests were used to observe an association between the qualitative study and outcome variables. All p values <0.05 were taken as significant. Statistical analysis was performed by using software SPSS version 17.
Twenty-four (9.37%) patients were diagnosed to have celiac disease; the mean age at diagnosis of diabetes was 9.34±7.3 years. Only one patient out of twenty four (0.041%) patients with celiac disease associated with type 1 diabetes had been diagnosed before the detection of diabetes mellitus.
Table 1 shows the comparison between the patients with and those without celiac disease, the age of presentation with celiac disease was almost one year later than the age of presentation of patients without celiac disease.
Click here to download Table 1Table 1. Baseline parameters between type 1 diabetes with and without celiac diseases.
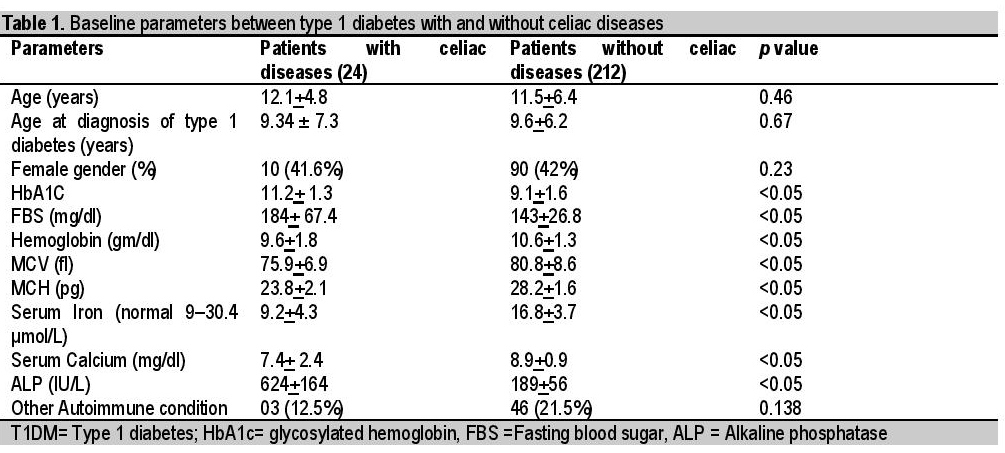
Patients with celiac disease had much higher HbA1C, FBS and ALP in comparison with patients without celiac disease, which are all significant (<0.05). However, celiac disease patients had lower hemoglobin, MCV, MCH, serum iron, and serum calcium and again, all were statistically significant (<0.05). Sex ratio was found to be equal in both, while the incidence of other autoimmune conditions was found to be insignificant.
Table 2 shows the demographic profile of patients with celiac disease and the most common manifestations. Some uncommon manifestations were also present in a small number of patients, these are rickets (20.8%), recurrent hypoglycemia (16.6%), carpopedal spasm (8.3%), and night blindness (8.3%).
Click here to download Table 2Table 2. Clinical profile of children with type 1 diabetes associated with celiac disease, N=24, Uttar Pradesh, India.
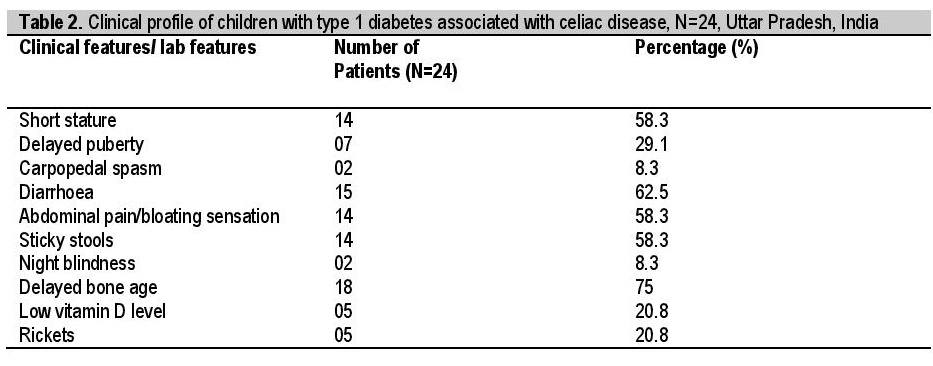
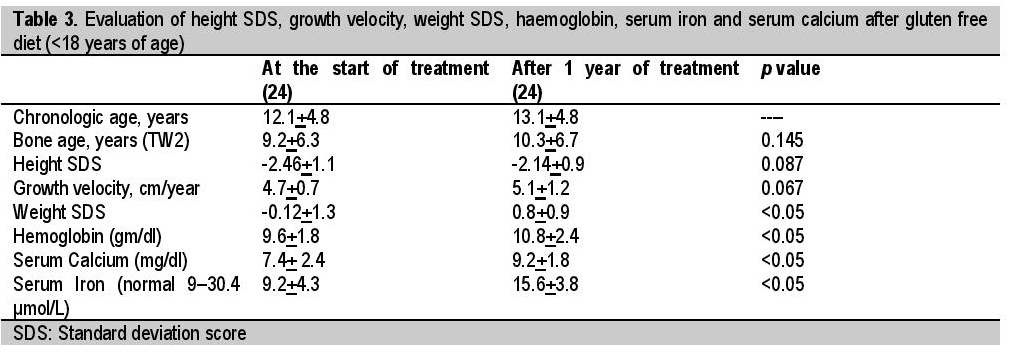
Table 3 shows the growth parameters and clinical characteristics of the 24 type 1 diabetes mellitus patients with celiac diseases (14 males and 10 females) less than 18 years of age enrolled in the study. Weight standard deviation score (SDS) increased from -0.12±1.3 at the start of gluten free diet to 0.8±0.9 after 12 months of study (p<0.05). Height SDS decreased from -2.46±1.1 at the start of gluten free diet to -2.14±0.9 after 12 months (p=0.087). Bone age SDS increased from 9.2±6.3 at the start of gluten free diet to 10.3±6.7 after 12 months. Height velocity increased from 4.7±0.7 cm/year in the year before treatment to 5.1±1.2 cm/year during treatment (p= 0.05). Hemoglobin, serum calcium and serum iron all increased significantly (p<0.05).
Click here to download Table 3Table 3. Evaluation of height SDS, growth velocity, weight SDS, haemoglobin, serum iron and serum calcium after gluten free diet (<18 years of age).
Patients were divided into three groups: Prepubertal (7), pubertal (7 patients, either with short stature or other clinical feature of celiac disease), and postpubertal (10, seven with delayed puberty and three with age more than 14 years, normal puberty but height less than 2SD). Of 7 patients in the prepubertal age group, only 1 patient attained puberty, the rest of the patients remain prepubertal. In the postpubertal patients, 3 out of 7 patients attained the puberty; and in the rest of the cases there was improvement in height and growth velocity. Besides the gluten free diet, other confounding factors which might contribute to clinical results might be pubertal growth spurt, good nutrition, better education, motivation, and presence of other autoimmune disorders.
After 1 year of follow-up, there was a signi?cant increase in weight SDS (p<0.05), whereas the increase in height SDS (p=0.087) did not reach statistical signi?cance. Height velocity increased from 4.7±0.7 cm/year in the year before treatment to 5.1±1.2 cm/ year during treatment (p=0.05).
This is a prospective observation study carried out in the Department of Endocrinology and Metabolism during the 2 year study period from July 2011 to June 2013.
Celiac disease is an autoimmune-mediated enteropathy precipitated by the ingestion of gluten-containing foods (including wheat, rye and barley) in genetically susceptible persons. Celiac disease is also frequently associated with type 1 diabetes mellitus but less frequently than autoimmune thyroiditis. During the last few years, numerous screening studies conducted all over the world showed the increased celiac diseases prevalence in type 1 diabetes mellitus.5
However data from South Asia is very limited, especially in the Indian subcontinent.9 Its prevalence in children and adolescents with type 1 diabetes ranges from 5 to 7%, the previous study done by Bhadada SK et al.,10 showed the prevalence rate of 11.1% in type 1 diabetic population.
Although screening detected cases of celiac diseases in children with diabetes mellitus, the majority are reported to be asymptomatic or silent.11-13
Studies on the association of celiac diseases on glycemic control and growth in patients with T1D have shown conflicting results.13-14 In the present study, patients with type 1 diabetes with celiac disease had poor glycemic control and nutritional status as judged by fasting blood sugar, HBA1C, serum Ca, serum iron and growth velocity.
While the majority of our patients with celiac diseases were found to have no gastrointestinal symptoms, an index of malabsorption with iron deficiency, and hypocalcaemia were also prominent in the celiac disease patients.15 The potential for early reversal of abnormalities in indices of intestinal malabsorption (iron and calcium deficiencies) is one of the advantages for screening asymptomatic children for early detection of celiac diseases in T1D patients.
The predominance of male gender among celiac diseases patients in the present study has been also been observed in few studies;17 while other studies in different races have shown female predominance.16 The gender variation likely represents variability of genetic and environmental factors among different races.
Patients were educated on dietary modification chart, audio visual aids, continuous follow up visits, awareness about impact of nonadherence, anthropometric measurements and laboratory investigations. Poor weight gain, height and growth velocity after institution of a gluten free diet have been shown in a group of children with DM, suggesting that they struggled to eat a gluten free diet that is suitable for children with diabetes. We found that compliance with such a restricted diet was not easy in all children. However, our most important observation was a significant improvement in weight, height and growth velocity in those children who were compliant with the diet, but not in those who continued to eat gluten.
After 1 year of follow-up, there was a signi?cant increase in weight SDS (p<0.05), whereas the increase in height SDS (p=0.087) did not reach signi?cance. However, height velocity increased from 4.7±0.7 cm/year in the year before treatment to 5.1±1.2 cm/year during treatment (p=0.05). Haemoglobin, mean corpuscular volume, serum calcium and serum iron also increased significantly.
Numerous studies have shown the positive effect of gluten-free diet on increased weight, height and growth velocity18 as well as on serum calcium, serum ferritin and haemoglobin.19 Moreover improvement of bone status in patients with type 1 diabetes mellitus with adherence to gluten-free diet has been reported.20
Patients with celiac disease associated with type 1 diabetes mellitus frequently have poor glycemic control and impairment in several growth parameters. When these patients are put on gluten restricted diet, they show signs of improvement in the term of weight gain, height, serum Ca, serum iron, haemoglobin, and in height velocity.
LimitationsThe improvement in the growth parameters may not be explained by the gluten free diet alone, but also other confounders such as pubertal growth spurt, good nutrition, better education, motivation, and presence of other autoimmune disorder in the patient. As a limitation of this study, the impact of these confounders and its interaction with the gluten free diet was not investigated.
Statement of AuthorshipAll authors have given approval to the final version submitted.
Author DisclosureAll the authors declared no conflicts of interest.
Funding SourceNone.
1. Cappa M, Bizzarri C, Crea F. Autoimmune thyroid diseases in children. J Thyroid Res.2010;2011:675703. http://dx.doi.org/10.4061/2011/675703.
2. Kakleas K, Karayianni C, Critselis E, Papathanasiou A, Petrou V, Fotinou A, et al. The prevalence and risk factors for coeliac disease among children and adolescents with type 1 diabetes mellitus. Diab Res ClinPract. 2010;90(2):202-8. http://dx.doi.org/10.1016/j.diabres.2010.08.005. 3. Mäki M, Mustalahti K, Kokkonen J, Kulmala P, Haaplahti M, Karttunen T, et al. Prevalence of celiac disease among children in Finland. N Engl J Med. 2003; 348: 2517-24. http://dx.doi.org/10.1056/NEJMoa021687. 4. Gutch M, Kumar S, Saran S, Gupta KK, Mohd Razi S, Philip R. Prevalence of autoimmune disorders in pediatrics type-1 diabetes mellitus in Western Uttar Pradesh, India. Int J Med Public Health. 2015;5(1):29-31. http://dx.doi.org/10.4103/2230-8598.151246. 5. Gujral N, Freeman HJ, Thomson ABR. Celiac disease: Prevalence,diagnosis, pathogenesis and treatment. World J Gastroenterol. 2012;18(42):6036-59. http://dx.doi.org/10.3748/wjg.v18.i42.6036. 6. Rojas-Villarraga A, Amaya-Amaya J, Rodriguez-Rodriguez A, Mantilla RD, Anaya JM. Introducing polyautoimmunity: Secondary autoimmune diseases no longer exist. Autoimmune Dis. 2012;2012:254319. http://dx.doi.org/10.1155/2012/254319. 7. Sukriti K,Manish G, Syed RM, Abhinav GK, Keshav GK,Tugveer AS. Prevalence and clinical profile of celiac disease in patients with type 1 diabetes mellitus in Western Uttar Pradesh, India. J ASEAN Fed Endocr Soc. 2015;30(2):142-6. http://dx.doi/org/10.15605/jafes.030.02.02. 8. Galluzzi F, Stagi S, Salti R, Toni S, Piscitelli E, Simonini G, et al. Osteoprotegerin serum levels in children with type 1 diabetes: A potential modulating role in bone status. Eur J Endocrinol. 2005;153(6):879-85. http://dx.doi.org/10.1530/eje.1.02052. 9. Cerruti F, Bruno G, Chiarelli F, Lorini R, Meschi F, Sacchetti C and the Diabetes Study Group of the Italian Society of Pediatric Endocrinology and Diabetology. Younger age at onset and sex predict celiac disease in children and adolescents with type 1 diabetes: An Italian multicenter study. Diabetes Care. 2004;27(6):1294-98. http://dx.doi.org/10.2337/diacare.27.6.1294. 10. Bhadada SK, Kochhar R, Bhansali A, Dutta U, Kumar PR, Poornachandra KS, et al. Prevalence and clinical profile of celiac disease in type 1 diabetes mellitus in north India. J Gastroenterol Hepatol. 2011;26(2):378-81. http://dx.doi.org/10.1111/j.1440-1746.2010.06508.x. 11.Goh C, Banerjee K. Prevalence of coeliac disease in children and adolescents with type 1 diabetes mellitus in a clinic based population. Postgrad Med J. 2007;83(976): 132-6. http://dx.doi.org/10.1136/pgmj.2006.049189. 12. Bashiri H, Keshavarz A, Madani H, et al. Celiac disease in type-1 diabetes mellitus: Coexisting phenomenon. J Res Med Sci. 2011;16:401-6. 13. Amin R, Murphy N, Edge J, Ahmed ML, Acerini CL, Dunger DB. A longitudinal study of the effects of a gluten-free diet on glycemic control and weight gain in subjects with Type 1 diabetes and celiac disease. Diabetes Care. 2002;25(7):1117-22. http://dx.doi.org/10.2337/diacare.25.7.1117. 14. Kaspers S, Kordonouri O, Schober E, Krause U, Schimmel U, Hauffa BP, et al. Anthropometric parameters, metabolic control and thyroid autoimmunity in 127 biopsy-positive patients with type 1 diabetes and coeliac disease (CD) compared to 18,470 diabetic subjects without CD. 18th Congress of the International Diabetes Federation, Paris, 24-29. Diabetologia. 2003;46(S2):A232-3(presentation 671). 15. Buysschaert M, Tomasi JP, Hermans M. Prospective screening for biopsy proven coeliac disease, autoimmunity and malabsorption markers in Belgian subjects with type 1 diabetes. Diabet Med. 2005;22(7):889-92. http://dx.doi.org/10.1111/j.1464-5491.2005.01542.x. 16. Shahbazkhani B, Faezi T, Akbari MR, Mohamadnejad M, Sotoudeh M, Rajab A, et al. Coeliac disease in Iranian type I diabetic patients. Dig Liver Dis. 2004;36(3):191-4. http://dx.doi.org/10.1016j.dld.2003.10.015. 17. Araújo J, da Silva GAP, de Melo FM. Serum prevalence of celiac disease in children and adolescents with type 1 diabetes mellitus. J Pediatr (Rio J).2006;82:210-14. http://dx.doi.org/10.2223/JPED.1478. 18. Goh VL, Estrada DE, Lerer T, Balarezo F, Sylvester FA. Effect of gluten-free diet on growth and glycemic control in children with type 1 diabetes and asymptomatic celiac disease.J Pediatr Endocrinol Metab. 2010;23(11):1169-73. http://dx.doi.org/10.1515/jpem.2010.183. 19. Hansen D, Brock-Jacobsen B, Lund E, Bjørn C, Hansen LP, Nielsen C, et al. Clinical benefit of a gluten-free diet in type 1 diabetic children with screening-detected celiac disease: A population-based screening study with 2 years' follow-up. Diabetes Care. 2006;29(11): 2452-56. http://dx.doi.org/10.2337/dc06-0990. 20. Valerio G, Spadaro R, Iafusc, D, Lombardi F, del Puente A, Esposito A, et al. The influence of gluten free diet on quantitative ultrasound of proximal phalanxes in children and adolescents with type 1 diabetes mellitus and celiac disease. Bone. 2008;43(2):322-26. http://dx.doi.org/10.1016/j.bone.2008.04.004.Authors are required to accomplish, sign and submit scanned copies of the JAFES Author Form consisting of: (1) the Authorship Certification that the manuscript has been read and approved by all authors, and that the requirements for authorship have been met by each author, (2) the Author Declaration that the article represents original material that is not being considered for publication or has not been published or accepted for publication elsewhere, (3) the Statement of Copyright Transfer [accepted manuscripts become the permanent property of the JAFES and are licensed with an Attribution-Share Alike-Non-Commercial Creative Commons License. Articles may be shared and adapted for non-commercial purposes as long as they are properly cited], (4) the Statement of Disclosure that there are no financial or other relationships that might lead to a conflict of interest. For Original Articles involving human participants, authors are required to submit a scanned copy of the Ethics Review Approval of their research. For manuscripts reporting data from studies involving animals, authors are required to submit a scanned copy of the Institutional Animal Care and Use Committee approval. For Case Reports or Series, and Images in Endocrinology, consent forms, are required for the publication of information about patients; otherwise, authors declared that all means have been exhausted for securing such consent. Articles and any other material published in the JAFES represent the work of the author(s) and should not be construed to reflect the opinions of the Editors or the Publisher.