Diabetes is the classic chronic disease that requires a multidisciplinary care team approach to provide comprehensive management to reduce complications, both acute as well as in the long-term.
The Diabetes Care model in Malaysia is continuing to evolve. Approximately 80% of people with diabetes seek treatment from the Ministry of Health. As such, it is appropriate that the Malaysian Health Ministry, Disease Control Division, is spearheading the initiative to develop a functioning Diabetes Care model and will continue to drive its establishment and success. Before moving forward, it is important to recognise where we are at this moment. Several points need to be considered, that include:
- Burden of Disease
- Structure of the healthcare system
- Where are the people seeking care
- How are we doing (recent audits, including DiabCare, etc.)
- Diabetes care team - what is already in place and what needs to be done
- National guidelines for diabetes management
- Strategies for prevention
Burden of disease
Malaysia continues to progress as a nation, both socially and economically. Concomitant with this progress, disease patterns and burdens have changed to reflect these changes in lifestyle and dietary patterns. Unfortunately, of all the countries in the ASEAN region, Malaysia probably has the distinction of having the highest prevalence of diabetes. The recent National Health and Morbidity Survey conducted in 2011,1 found that 20.8% of Malaysians above the age of 30 years had diabetes (10.7% known and 10.1% undiagnosed). With a population of 30 million, that would mean that there are approximately 2.6 million Malaysians with diabetes.
Structure of the healthcare system and where are the people seeking care
As in most developing nations, the healthcare system is broadly divided into hospital-based and outpatient, primary care-based facilities.
In order to plan proper diabetes care managements to address the needs of this population of individuals, we need to know where they are seeking their medical care.
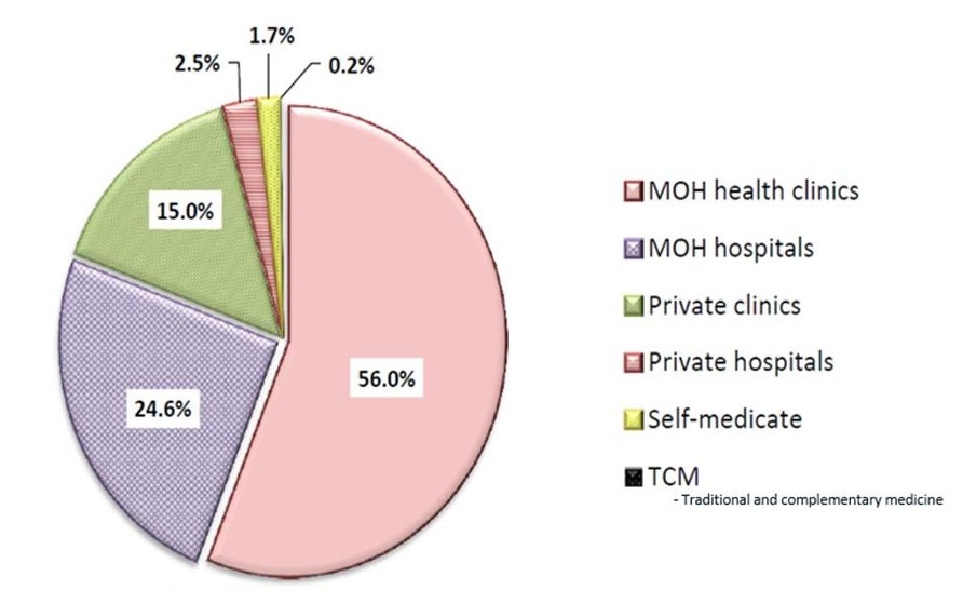
In Figure 1, we recognise that 80% of people with diabetes are seeking care in the primary care health clinics (56%) and hospital-based clinics (24.6%) in the Ministry of Health (MOH). As such, much of the Diabetes Care model has to be designed around the Ministry of Health, in particular, the primary care clinics, that are carrying much of the burden.2
Click here to download Figure 1Figure 1. Usual place of treatment of patients diagnosed with diabetes in Malaysia.
How are we doing? National Diabetes Registry3 and DiabCare4
The national diabetes registry started in 2009 and went web-based on January 2011. It supported the implementation of the annual "Diabetes Clinical Audit" amongst patients with Type 2 Diabetes attending the MOH health clinics/primary care facilities. Over 2009-2012, ~650,000 patients' data were added into this registry. Mean age of the patients was 59.7 years. HbA1c was performed in 78% of the patients (in 2012), with the mean HbA1c of 8.1% for T2DM,1 of which 37.9% of patients achieved target HbA1c <7.0%. The mean BMI was 27.4 kg/m2 and only 16.6% achieved BMI <23 kg/m2. Among these patients with T2DM, 70.1% had hypertension and 55.1% had dyslipidaemia. The most common DM-related complications were nephropathy (7.8%), retinopathy (6.7%), and ischaemic heart disease (5.3%).
For tertiary hospital-based diabetes management, Diabcare 20082 assessed ~1549 patients with T2DM attending the outpatient diabetes clinics of the general hospitals and institutional academic hospitals, the mean HbA1c was 8.66%, of which only 22.0% had HbA1c <7.0%. In the latest 2013 Malaysian DiabCare audit, 1668 patients with T2DM assessed from the same hospital-based diabetes clinics had a mean HbA1c of 8.52%, with a similar 23.7% achieving HbA1c <7.0% (unpublished data).
These results continue to emphasise the fact that achieving glycaemic control in our diabetic population remains a challenge.
Diabetes Care Team - what is already in place and what needs to be done
There are many models of integrated diabetes care. The main objective of these Diabetes Care models is to establish pathways to provide improved patient care and allow appropriate and timely referral of patients between different parts of the healthcare system. However there remain significant barriers that need to be overcome.
Key members of the multidisciplinary team needed to ensure success of the Diabetes Care model, include diabetologists or endocrinologists / internal medicine physicians / family medicine specialists (FMS) / medical officers, certified diabetes nurse educators / nurse practitioners, pharmacists, as well as dietitians. Other members (if available) include podiatrists, optometrists, dental care professionals and mental health professionals. Currently, in Malaysia, there are endocrinologists / internal medicine physicians in every state general hospital offering specialist diabetes care services. For the smaller hospitals, there are internal medicine physicians handling that aspect. Each of these main general hospitals have established diabetes resource centres, where there are diabetes nurse educators helping to deliver patient-centered education to inpatients as well as outpatients. The Ministry of Health pharmacists have also initiated services that offer education focusing primarily on medications, how the medications work with emphasis on the importance of adherence / compliance. This initiative was started in 2006, with formation of the Diabetes Mellitus Treatment Adherence Clinics (DMTAC),5 coordinated and operated by pharmacists. After being shown to improve glycaemic control on follow-up,5 these services have been expanded from the major public hospitals to the primary care clinics.
Family medicine specialists (FMS) form the backbone of the health clinics that look after ~60% of the diabetes population. The Ministry of Health (MOH) has 960 primary care clinics; and there are only ~280 trained and certified FMS' "manning" these clinics. There is a continuing need to train more FMS' to fill this huge void. These trained FMS' further improve care by providing downstream educational courses to update trainee medical officers. They also continue to audit diabetes care and initiate patient educational initiatives. There is also no official integration or pathways between these health clinics and the major public hospitals or institutional hospitals where many of the physicians and endocrinologists practice to enable more timely and seamless transfer of patients requiring complex care between these systems.
Certified diabetes educators (DNEs) are an essential member of this diabetes care team. On an individual basis, they are able to educate patients on medications, particularly insulin injection techniques, timing of injections; and in addition, organise small group educational initiatives to allow for broader coverage of patients attending the outpatient diabetes facilities. Currently, only the major urban hospitals have such DNEs, while there are no such individuals to help drive a systematic diabetes service in smaller hospitals and rural healthcare facilities.
Dietitians are also important members of the team, and for best results, they should be available at the diabetes outpatient clinics so that patients can be seen and appropriate advice given with input from the doctors. There are currently approximately 39,000 registered dietitians working in the MOH primary health clinics. Unfortunately, there are still some areas and clinics, particularly in the rural areas, that have no dietitian support. The Malaysian Dietitians' Association has been actively supporting the management of patients with diabetes. With this in mind, they have helped develop the nutrition chapter of the Malaysian Clinical Practice Guideline (2009,6 with an update expected in December 2015). They have also developed 2 guidelines; Medical Nutrition Therapy guidelines for Type 2 diabetes mellitus, in 2005,7 updated in 2013.8 Of course, training specialist dietitians with in-depth knowledge of dietetic management for Type 1 diabetes, diabetes in pregnancy / gestational diabetes or concomitant renal dysfunction will enhance their contribution to the Team.
There are no certified trained podiatrists available to help in the important aspect of diabetes foot care. Several of the main hospitals have diabetes foot services, largely manned by orthopaedic surgical units and orthopaedic surgical doctors. This lack needs to be addressed.
Important Role of Disease Control Division, Ministry of Health
The MOH has a unit in the Non-communicable Disease (NCD) Section of the Disease Control division (DCD), which plans initiatives for the management of chronic diseases like diabetes. They have a team that is dedicated to planning strategies, implementation of appropriate programs, educational initiatives and obtaining funding; with the end result - setting-up of a successful chronic care model for diabetes. The NCD section developed a National Strategic Plan for Non-communicable Diseases in 2010,9 presented and approved by the Cabinet of the Government of Malaysia. This provided a framework for strengthening NCD prevention and control in Malaysia. In addition, systematic management of NCDs at the community level (that included diabetes) was implemented - with 7 goals/targets, including: screening, registration, clinical management, complications screening, rehabilitation, defaulter tracing, and self-care / patient empowerment.
In addition, the disease control division has recognised the importance of improving healthcare delivery; as well as aligning finances. This division works toward obtaining funding allocation for human resource development eg. Diabetes Nurse Educators as well as funding to enable timely availability of medication to achieve glucose targets.
Newer modalities of anti-diabetic medications, including oral dipeptidyl-peptidase inhibitors (DPP-4i), sodium glucose co-transporter 2 inhibitors (SGLT2-inhibitors), modern insulin analogs (insulin aspart, lispro insulin, insulin glargine, etc.) have all been registered in a timely fashion in the national drug formulary for use; and budgets were made available for prescription to appropriate patients attending the public MOH clinics.
With regard to patient empowerment, modules for patient health education, including pre- and post-test questionnaires, have been developed and published by the Disease Control Division, MOH. Further development of a Peer Support Group educational initiative has been developed and trial runs have proven its success. It remains for this initiative to be rolled out to the wider public.
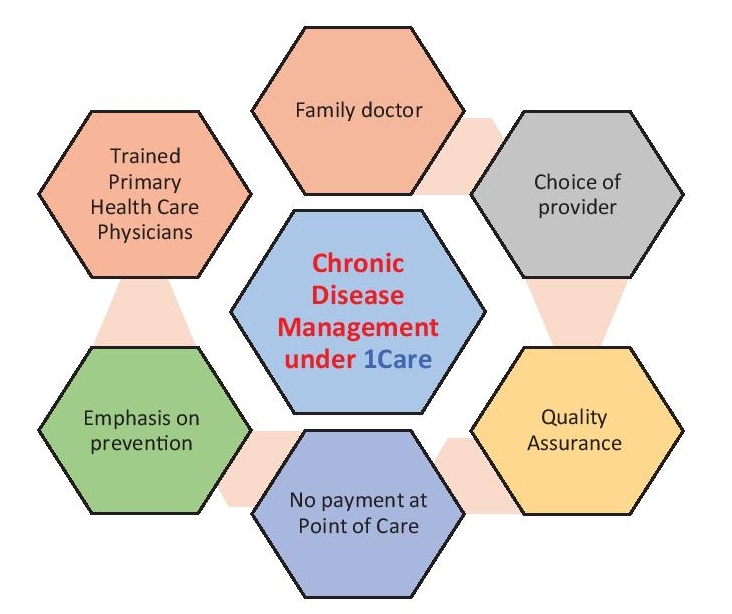
Recognising that majority of patients with diabetes are accessing care from primary care facilities in the MOH, there are also proposed reforms to integrate public and private healthcare sectors, as shown in Figure 2. This will devolve some of the healthcare burden to the private clinics that are abundant in the whole country and further improve overall healthcare.
Click here to download Figure 2Figure 2.Proposed structural reform to integrate public and private healthcare sectors (Malaysia).
Unfortunately, despite having many of the members of this multidisciplinary team as mentioned above, there remains significant fragmentation of these services. These services need to be integrated to allow for timely referrals to improve patient experiences and outcomes.
Malaysia has been extremely fortunate in that the MOH-DCD has been very supportive, working closely with other stakeholders in diabetes, e.g. NGOs and academic diabetes fraternity to drive change for the improvement of diabetes care in the country.
Much of the initiatives, programs, developments described above have been driven by the Ministry of Health, with some minor assistance from the endocrinologists, physicians, dietitians and pharmacists, helping with clinical audits and the clinical practice guidelines.
National Guidelines for Management of T2DM
Clinical Practice Guidelines (CPGs) have been developed over the past 15 years and in December 2015, the latest 5th CPG for T2DM will be rolled out. Updated CPGs are required to allow timely changes to recommendations for improving diabetes care and aligning clinical decision making according to prevailing evidence. These guidelines are endorsed by the MOH and made available to all practising physicians. In addition, there is a specific insulin initiation guideline to assist primary care doctors.
Strategies for Prevention
Of course, prevention strategies cannot be excluded from any future plans for diabetes care. Again, the Ministry of Health recognizes this and has initiated collaborative efforts with a "Whole-of-Government" strategy to engage relevant ministries such as Ministry of Environment / Infrastructure, Ministry of Transport as well as local governments to modify behaviour of the population toward a healthy lifestyle. These are spelt out in the NSP-NCD.9
The burden of diabetes has increased exponentially in Malaysia and achieving glycaemic control remains a challenge. There is an increasing challenge in providing satisfactory, consistent quality of care across a broad range of patients. Many of the specialized services are located in the urban areas, in the major public hospitals and institutional centres. Referrals to specialists are delayed due to late diagnosis and sub-optimal control. Timely referrals with more seamless transition within the healthcare system needs to be established. Patient-related factors, i.e. patient empowerment, need to be addressed. Continued close collaboration between the MOH and other key stakeholders, such as non-governmental organisations (e.g. Diabetes Malaysia / Malaysian Diabetes Educator Society / National Diabetes Institute) as well as corporate partners - will help drive many of these changes required to further establish a successful Diabetes Care model in Malaysia.
After decades of establishing a comprehensive healthcare system, Malaysia continues to work toward improving its chronic disease care models, in particular, for the management of people with diabetes. The component that needs urgent attention would be the recognition of the Certified Diabetes Nurse Educator (DNE) - to recognise the DNE as a specialised field of nursing, allowing definitive career opportunities and appropriate remuneration. These steps would encourage more healthcare professionals to embark on training as DNEs.
Being a developing nation, Malaysia has come a long way toward providing quality medical care to its populace. After establishing good acute care services, attention is needed toward chronic disease management. With the high prevalence of diabetes, it is essential that an Integrated Diabetes Care model be put in place to handle the demands and to improve patient outcomes. What is desperately required are more well-trained certified diabetes nurse educators to help drive these initiatives through, with emphasis on patient education and patient self-empowerment.
The Disease Control Division (Non-communicable Disease Section) of the Ministry of Health has been supportive and will continue to drive change and progress toward achievement of this goal.
Acknowledgment
I would like to thank Drs. Feisul Idzwan Mustapha, Fatanah Ismail of the Non-Communicable Disease Section, Disease Control Division, Department of Public Health, Ministry of Health, Putrajaya for their kind assistance.
1. Feisul M. Current burden of diabetes in Malaysia. In: Proceedings of the 1st National Institutes of Health (NIH) Scientific meeting; June 2012; Selangor, Malaysia.
2. Institute of Public Health (IPH). The 4th National Health and Morbidity Survey (NHMS IV). Vol II: Non-communicable Diseases. National Diabetes Registry Report Volume 1 2009-2012, ISBN 978-967-0399-53-9. 3. National Diabetes Registry Report, Volume 1, 2009-2012; Ministry of Health Malaysia; 2013 Jul. Available on http://www.moh.gov.my/index.php/pages/view/115. 4. Mafauzy M, Zanariah H, SP Chan. Med J Malaysia. 2011;66(3):175-181. 5. Lim PC, Lim K. Evaluation of a pharmacist-managed diabetes medication therapy adherence clinic. Pharm Pract (Granada). 2010;84(4):250-254. 6. Clinical Practice Guideline for Management of Type 2 diabetes mellitus, 4th edition. 2009. www.moh.gov.my/attachments/3878.pdf. Accessed 24 October 2015. 7. Malaysian Dietitians' Association. Medical Nutrition Therapy guidelines for Type 2 diabetes mellitus. 1st ed. Ministry of Health, 2005. 8. Malaysian Dietitians' Association. Medical Nutrition Therapy guidelines for Type 2 diabetes mellitus. 2nd ed. Ministry of Health, 2013. 9. MOH Malaysia: National Strategic Plan for non-communicable disease 2010-2014. http://www.moh.gov.my/images/gallery/nspncd.Authors are required to accomplish, sign and submit scanned copies of the JAFES Declaration that the article represents original material that is not being considered for publication or has not been published or accepted for publication elsewhere.
Consent forms, as appropriate, have been secured for the publication of information about patients; otherwise, authors declared that all means have been exhausted for securing such consent.
The authors have signed disclosures that there are no financial or other relationships that might lead to a conflict of interest. All authors are required to submit Authorship Certifications that the manuscript has been read and approved by all authors, and that the requirements for authorship have been met by each author.