The global prevalence of type 2 diabetes mellitus is rapidly increasing as a result of population ageing, urbanization and its associated lifestyle changes. Its prevalence has more than doubled over the past three decades.1 In 2014, the global prevalence of diabetes was estimated to be 9% among adults, where 90% were considered as having type 2 diabetes.2 By 2030, the prevalence is expected to increase to 7.7% affecting 439 million adults. Between 2010 and 2030, there will be a 69% increase in the number of adults with type 2 diabetes in developing countries and a 20% increase in developed countries.3 In Asia, similar epidemiologic trends are being seen as more Asians adopt a westernized lifestyle. The Philippines is a country considered to have a high prevalence of type 2 diabetes, with an estimated 7.8 million cases and is projected to be ranked 9th overall by 2030.2 In a recent local study, the 9-year incidence of type 2 diabetes was 16.3% while its prevalence was 28.0%.4
Diabetes mellitus is a chronic metabolic disorder characterized by a deficiency in insulin secretion or an increased insulin resistance, resulting in hyperglycemia. Type 2 diabetes (formerly called non-insulin-dependent or adult-onset) in particular results from the body's ineffective use of insulin and is largely the result of excess body weight and physical inactivity.5 People with type 2 diabetes, especially when it is poorly controlled, have an increased susceptibility to chronic infections and inflammation of oral tissues, including periodontal diseases (chronic gingivitis and periodontitis), dental caries, and oral candidiasis. This contributes to substantial oral functional disability.6 Oral complications are seen in 1/3 of people with type 2 diabetes.7
Type 2 diabetes is considered a risk factor for the development of periodontitis which is now considered to be the sixth complication of both type 1 and type 2 diabetes.8-9 Severe periodontitis was more often found in patients with type 2 diabetes (60% vs 39%).10 The likelihood of periodontitis among type 2 diabetics was 3 times greater than the general population, and progresses rapidly when poorly controlled.11 Majority of well-controlled studies showed a higher prevalence and severity of periodontal disease in type 2 diabetes with similar local irritation including greater loss of attachment, greater alveolar bone loss, increased bleeding on probing, and increased tooth mobility resulting in tooth loss.12-15 Similar trends were found in a local study where prevalence of periodontitis was noted to be at 68.23%.16
Furthermore, poor perception of one's oral health status among people with type 2 diabetes had a strong negative impact on health-related quality of life.17-18 Therefore, people with type 2 diabetes must be educated about the importance of removing oral plaque daily through meticulous oral hygiene, managing mouth dryness and diet, ceasing tobacco use and obtaining regular professional dental care and cleaning.6 The early detection and treatment of periodontal disease has led to improved glycemic control in patients with type 2 diabetes9 and was also confirmed in a recent study from the Philippines.16
Adults with diabetes are less likely to consult a dentist than to seek consult with a health care provider for diabetes care.20 A Philippine study by Ofilada among Filipinos with type 1 diabetes revealed that financial insufficiency, fear and the lack of dentists who are willing to treat diabetic patients were the common barriers to dental care.21 Patients with type 2 diabetes were more likely to receive more recommended elements of diabetes care whereas routine dental check-ups were commonly missed. They were also more likely to have numerous follow-ups with health care providers for aggressive glycemic control.22 This provides an opportunity for health care providers to screen and educate patients regarding the possible oral complications that might develop.
Given the importance of good oral health among type 2 diabetes patients and the current outpatient encounters with health care providers, a simplified oral health screening questionnaire might be of use in assessing oral health status of all patients diagnosed with type 2 diabetes. This would translate to earlier detection and referral to a dental specialist which would then contribute to better glycemic control when treated. Currently, the International Diabetes Federation (IDF) guidelines on oral health recommends routine clinical screening questions as the basis for further referral and management by the dentist.23 The Philippine Dental Association and the UNITE for Diabetes Philippine clinical practice guidelines both recommend screening for clinical symptoms and early referrals to dental service for better oral care and management.24
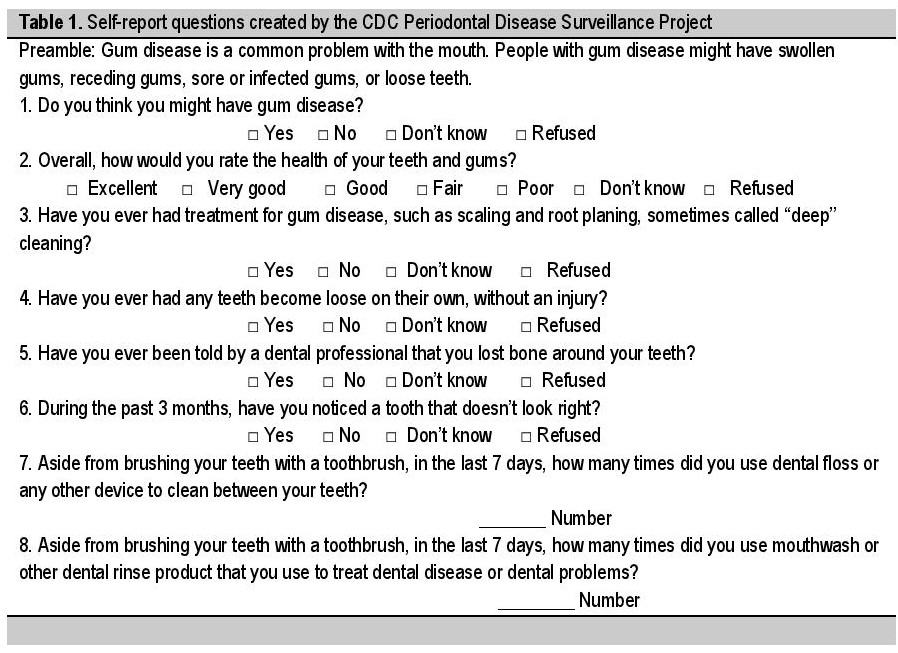
As of 2007, the Center for Disease Control and Prevention (CDC) in collaboration with the American Academy of Periodontology (AAP) has been working on the creation, formulation and evaluation of a self-report questionnaire in predicting the prevalence of periodontitis among adult population. Through a rigorous systematic process of selection and evaluation, the extensive CDC-AAP effort identified a set of eight self-report oral health questions that were considered promising for predicting the prevalence of periodontitis (Table 1).25 These eight oral health questions were previously selected and tested cognitively in United States adults where revisions were recommended (Table 2).26 An initial field assessment of these questions done in Australia demonstrated promising results for predicting the prevalence of periodontitis in adults.27 Similar assessment of these questions were validated in a pilot study done in the U.S. by Paul Eke and Bruce Dye.28 In addition to the oral health variables, several demographic and medical variables (age, sex, smoking history, education, diabetes duration, glycemic control) were also considered to be predictive of prevalence and severity of periodontitis.16,28
Click here to download Table 1Table 1. Self-report questions created by the CDC Periodontal Disease Surveillance Project
As of now, there is still no locally validated clinical oral health screening questionnaire. Application of the validated CDC self-reported oral health questionnaire can help in predicting diabetic patients at risk for periodontitis and warrant earlier dental consults. An inexpensive and easy tool for clinical assessment would be useful especially in a developing country like the Philippines where resources for health care access are limited. This paper aims for the following:
- To determine the prevalence and severity of periodontitis among patients with type 2 diabetes categorized according to tooth loss, medical and socio-demographic variables;
- To determine the response rates of patients with type 2 diabetes for each self-reported oral health questions;
- To determine the predictors of the seriousness of periodontitis among self-reported oral health variables, clinically determined number of teeth loss and socio-demographic and medical variables;
- To present a culturally accepted and validated self-reported oral health questionnaire and propose a scoring system that will predict severity of periodontitis among patients with type 2 diabetes.
Self-Reported Oral Health Questionnaire
The validated self-reported oral health questionnaire created by the CDC Periodontal Disease Surveillance Project was used in this study (Table 2). The content of the questionnaire was carefully translated into the Filipino language by expert linguists. One linguist translated the English questionnaire to Filipino, while another translated the Filipino version back to English. The resulting translation was then compared to the original English version for verification until a final Filipino version of the questionnaire was created.
Click here to download Table 2Table 2. Recommended revised questions for periodontal disease surveillance
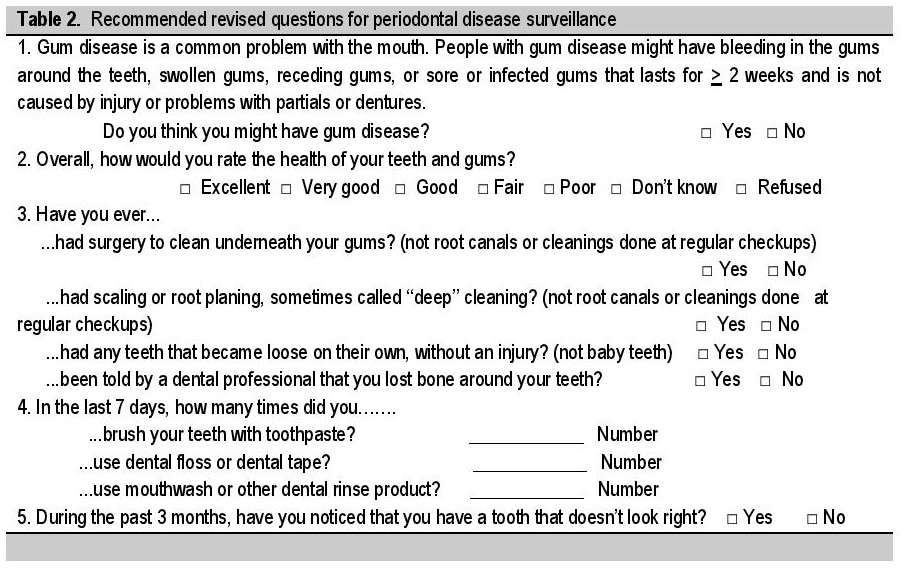
The translated Filipino version of the questionnaire was then incorporated with the original English version to create a questionnaire that would be expressed in two languages (English and Filipino). A pilot testing of the newly translated questionnaire was conducted with 20 Filipinos with type 2 diabetes who criticized and observed the applicability of the translated version. All suggestions, comments and criticisms were noted and resolved during the discussion thereby formulating a revised and improved version of the questionnaire.
Sample Size CalculationUsing PASS (Power Analysis and Sample Size) 2008 software, the minimum sample size requirement was computed using the parameters for logistic regression analysis: alpha (α) = 0.05, power (1-β) = 80%, X1 (percent of patients with tooth loss)= 67.6%, P0 (percent of periodontitis among patients without tooth loss)= 8.8%, P1 (percent of periodontitis among patients with tooth loss) = 30%. Except for the alpha level and power which were set by the reseachers, all other parameters were taken from the literature. The computed 136 minimum sample size was increased to 180 accounting for possible 20% non-response
Selection of ParticipantsInclusion Criteria
- Adult (Age ≥35 years) Filipino diagnosed with type 2 diabetes for at least 1 year. Diagnosis of Type 2 diabetes will be based on the American Diabetes Association criteria29 as follows: fasting blood sugar ≥126 mg/dl on 2 determinations; symptoms of hyperglycemia and random blood sugar ≥200 mg/dl; 2-hour plasma glucose ≥200 mg/dl after a 75 grams oral glucose tolerance test; standardized HbA1C ≥6.5%;
- Dentulous persons with ≥6 teeth present;
- Able to read, comprehend and respond to the series of questions;
- Willingness to undergo a dental examination.
Exclusion Criteria:
- Patients with heart murmurs that would require antibiotics prior to dental examination
This was a cross-sectional study conducted at the out-patient clinics of Philippine General Hospital. This study was reviewed and approved by the University of the Philippines Manila Research Ethics Board (UPMREB) Panel.
Potential study participants were provided with an overview of the study, its nature, purpose and significance. Once eligibility status was determined, recruited participants provided written informed consent (Appendix A) and contact information obtained. The interviewer then asked additional questions about gender, age, smoking status, education level, duration of diabetes and recent HbA1C level. Participants were then given the self-reported oral health questionnaire. All recruited patients were finally referred to a dentist for formal dental and periodontal evaluation. Results of the periodontal evaluation were given to the patient and subsequent intervention and follow up were advised accordingly to ensure proper treatment of periodontitis. All patient's data obtained were recorded individually using a patient data sheet while periodontal evaluation results were recorded using a separate dental sheet.
Click here to download Appendix AAppendix A. PATIENT'S INFORMED CONSENT: Validation of Self-Reported Oral Health Measures for Predicting Periodontitis Among Adult Filipinos with Type 2 Diabetes Mellitus

Periodontitis was determined from a full-mouth periodontal examination using the basic elements from the NHANES periodontal examination protocol. This included measuring gingival recession and probing depth (PD), to calculate loss of attachment, using a color-banded probe graduated at 2, 4, 6, 8, 10, and 12 mm. Measurements were made on six sites per tooth (mesio-buccal, buccal, distobuccal, mesio-lingual, lingual, and disto-lingual) for all teeth (excluding 3rd molars) by one examiner. Number of remaining teeth and lost teeth were also documented.30
VariablesFrom each participant, we collected socio-demographic and medical variables using a standard data collection form. Pertinent socio-demographic variables included age in years (specified as both continuous and categorical with two categories: 35-59, and ≥60), gender and educational attainment (high school graduate or lower and some college education or higher). Pertinent medical variables included cigarette smoking status (current smokers were subjects who had smoked ≥100 cigarettes in their lifetime and were currently smoking; former smokers were subjects who had smoked ≥100 cigarettes in their lifetime and not currently smoking; non-smokers were subjects who had not smoked =100 cigarettes in their lifetime),31 duration of diabetes (grouped into ≤10 years and >10 years), frequency of dental visits within a year and recent HbA1C level (within the last 3 months). Number of teeth remaining and number of teeth lost were also recorded and determined.
In this study, periodontitis was defined as a disease state in which there is an active destruction of the periodontal supporting tissues as evidenced by the presence of >3 mm probing depth and ≥3 mm periodontal attachment loss at the same site. Serious periodontitis was considered for participants fulfilling the criteria for moderate or severe periodontitis. Participants were classified according to severity of periodontitis using the following criteria (NHANES III protocol, 1988-1994):32
Severe periodontitis: 1) two or more teeth (or 30% or more of the teeth examined) having ≥5 mm probing depth, or 2) four or more teeth (or 60% or more of the teeth examined) having ≥4 mm probing depth, or 3) one or more posterior teeth with grade II furcation involvement.
Moderate Periodontitis: 1) one or more teeth with ≥5 mm probing depth, or 2) two or more teeth (or 30% or more of the teeth examined) having ≥4 mm probing depth, or 3) one or more posterior teeth with grade I furcation involvement and accompanied with ≥3 mm probing depth.
Mild periodontitis: 1) one or more teeth with ≥3 mm probing depth, or 2) one or more posterior teeth with grade I furcation involvement.
No periodontitis: persons with 6 or more teeth present who did not fulfill any of the above criteria.
Data AnalysisData analysis was done using the software Stata SE version 12. Different socio-demographic and medical variables, number of teeth lost and responses to self-reported oral health questionnaire were tabulated and recorded using descriptive statistics (mean, percentage). Multivariable logistic regression analyses were used to determine significant predictors that predicted the prevalence of serious periodontitis (created as moderate and severe disease versus mild and no disease combined). The predictive power of each variable was calculated and expressed using odds ratio, 95% confidence interval and p-value. The multivariate logistic regression analysis was then used to create a scoring system.
In total, 93.9% of the study participants had clinically defined periodontitis: 29.4% had mild periodontitis, 64.5% had serious periodontitis (moderate and severe periodontitis). Serious periodontitis was significantly higher among males, persons with low educational background, persons with current and smoking history, long diabetes duration, less frequent dental visits, poorly controlled glycemic state (Hba1c ≥7%) and persons who lost ≥6 teeth.
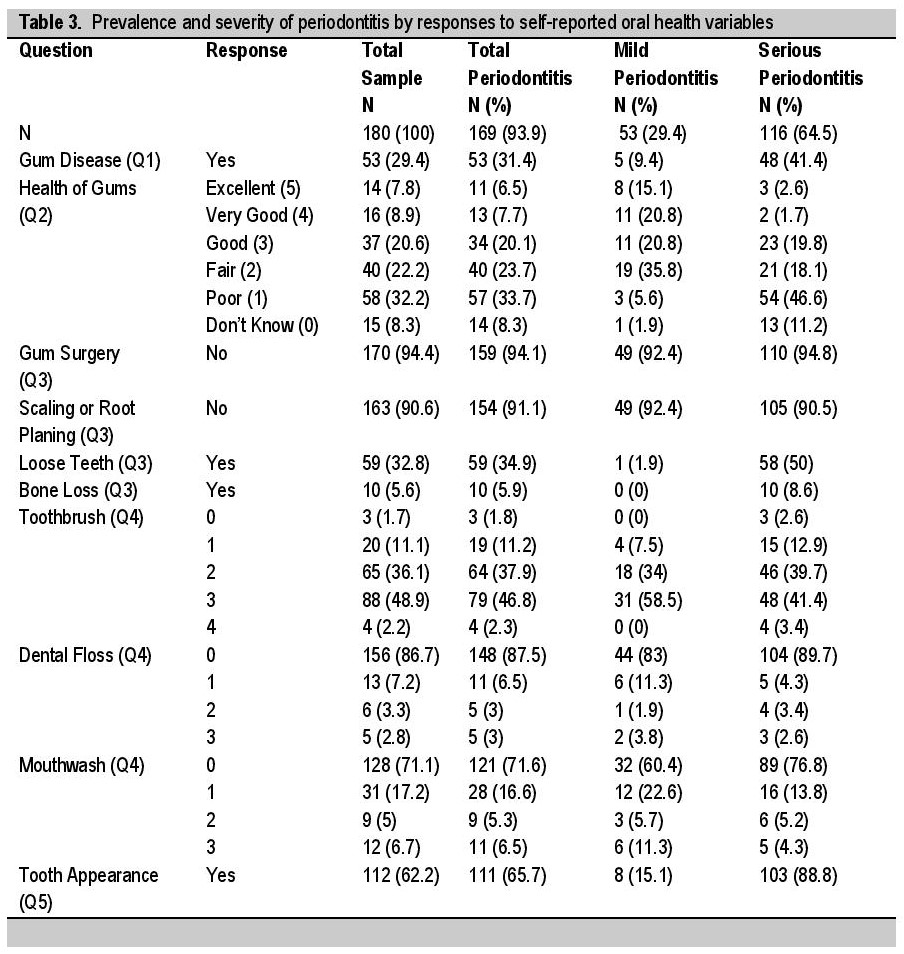
Table 3 summarizes the response rates to each self-reported oral health questions by periodontitis status. In general, understanding and responses to all oral health questions were very high and consistent. The states of gum health in question number 2 were converted to numerical equivalents upon recording ranging from 0 to 5. As observed, a bigger percentage of participants with serious periodontitis answered yes for gum disease (Q1), loose teeth (Q3), bone loss (Q3) and tooth appearance (Q5) while no for gum surgery (Q3) and scaling or root planing (Q3). Surprisingly, almost (>98.3%) all participants reported brushing their teeth regularly regardless of their eventual periodontitis state. On the other hand, most (>70%) did not report regular dental flossing and mouthwashing regardless of their final periodontal state. Majority of participants with serious periodontitis were also observed to report poor state of their gum health in response to question 2.
Click here to download Table 3Table 3. Prevalence and severity of periodontitis by responses to self-reported oral health variables
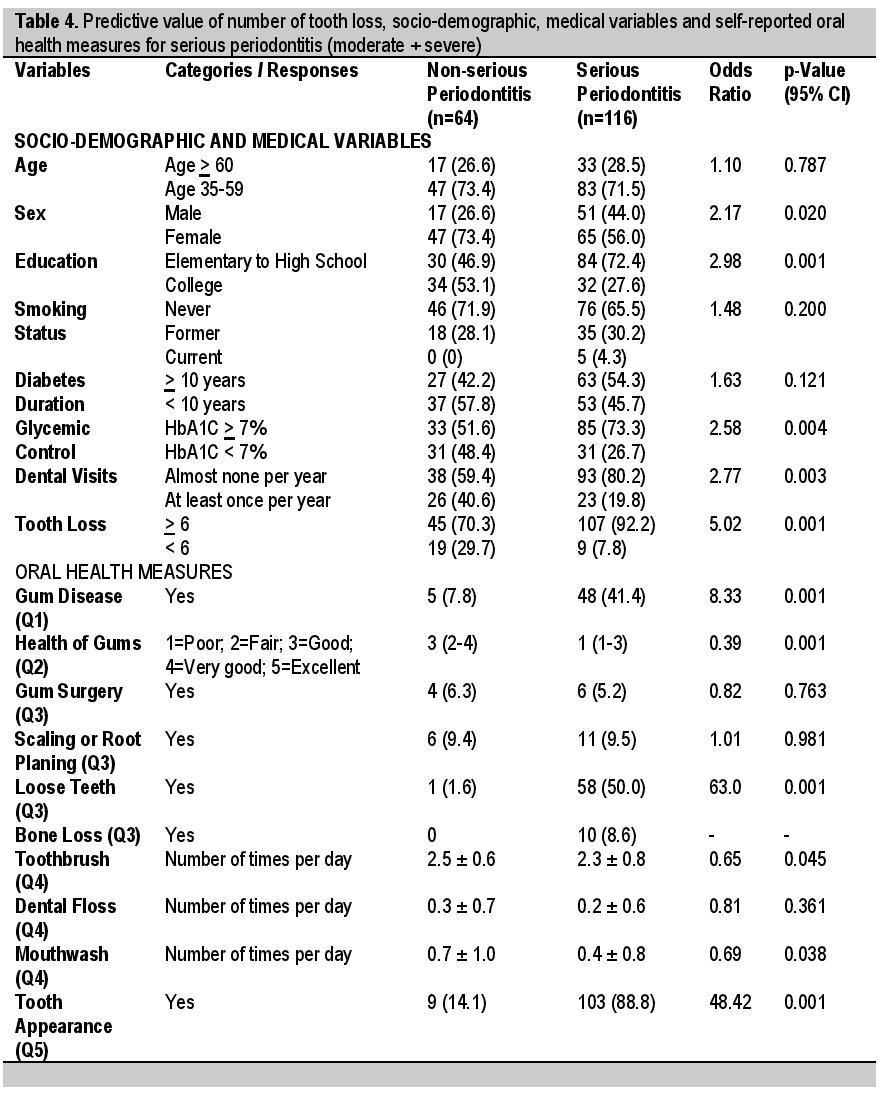
As shown in Table 4, socio-demographic and medical variables considered to be significantly predictive of serious periodontits were male sex [OR =2.17; 95%CI 1.12-4.35], low educational status [OR =2.98; 95%CI 1.57-5.63], poor glycemic control [OR =2.58; 95%CI 1.36-4.88], less frequent dental visits [OR =2.77; 95%CI 1.41-5.44] and teeth loss >6 [OR =5.02; 95%CI 2.11-11.94]. Self reported oral health variables shown to be significantly predictive of serious periodontitis included gum disease -Q1 [OR =8.33; 95%CI 3.11-22.30], state of gum health -Q2 [OR =0.39; 95%CI 0.28-0.54], loose teeth -Q3 [OR =63.0; 95%CI 8.45-469.58], brushing of teeth -Q4 [OR =0.65; 95%CI 0.43-0.99], use of mouthwash -Q4 [OR = 0.69; 95%CI 0.49-0.98] and poor tooth appearance -Q5 [OR = 48.42; 95%CI 19.48-120.38].
Click here to download Table 4Table 4. Predictive value of number of tooth loss, socio-demographic, medical variables and self-reported oral health measures for serious periodontitis (moderate + severe)
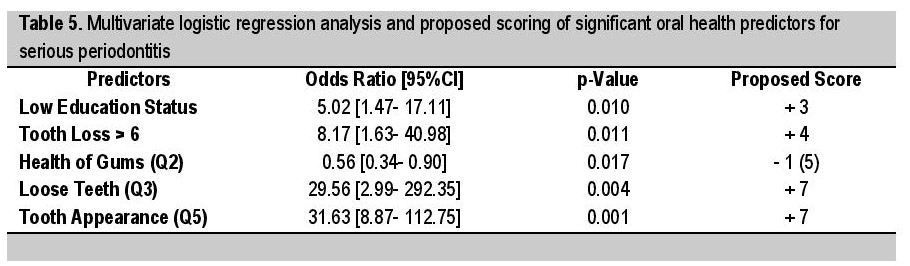
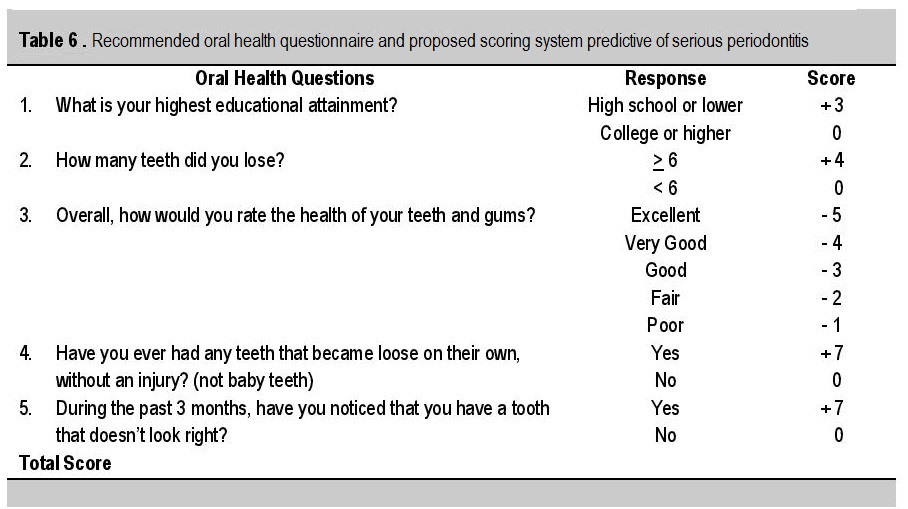
All predictor variables were combined in a single model using a multivariate logistic regression analysis to determine the performance of significant predictive factors in predicting periodontal state. As shown in Table 5, only low educational status [OR =5.02; 95%CI 1.47-17.11], teeth loss >6 [OR =8.17; 95%CI 1.63-40.98], state of gum health -Q2 [OR = 0.56; 95%CI 0.34-0.90], presence of loose teeth -Q3 [OR =29.56; 95%CI 2.99-292.35] and poor tooth appearance -Q5 [OR =31.63; 95%CI 8.87-112.75] were significant predictors for serious periodontitis. A recommended set of questions and proposed scoring system based on the logistic regression analysis of each predictor's strength was then formulated. Total score ranged from (-5) considered least likely to have serious periodontitis to (+20) considered most likely to have serious periodontitis (Table 6).
Click here to download Table 5Table 5. Multivariate logistic regression analysis and proposed scoring of significant oral health predictors for serious periodontitis
Click here to download Table 6
Table 6. Recommended Oral Health Questionaire and Proposed Scoring System Predictive of Serious Periodontitis
Overall, the results of this study showed that the self-reported oral health questionnaire was specific and valid in predicting serious periodontitis. This is expected as the presence of type 2 diabetes is already a risk for the presence of periodontitis.9-11,16 The higher prevalence of periodontitis (94% vs 68%) among the participants with type 2 diabetes in this study can be attributed to the socioeconomic status of patients seen in our institution that mostly caters to the indigent population of the country.16
Screening patients with serious periodontitis seems to be a more clinically relevant application as these patients would warrant immediate dental referral. A single model where all of the predictive factors were included and analyzed appeared to be the most predictive and useful.28 Misclassification of periodontal disease in this study was minimized using a full mouth periodontal examination "gold standard" which resulted in reduction in errors in our validity assessments.
The state of gum health appeared to be a protective predictive factor for both the presence and seriousness of periodontitis. A score of (-) 5 for excellent gum health and (-) 1 for poor gum health was used for easier scoring. Several dental hygiene practices like brushing teeth, dental flossing and use of mouthwash did not appear to be predictive of periodontitis since other local practices like betel nut chewing and use of toothpicks were reported. Low educational status was the only demographic variable found to be a significant predictive factor for serious periodontitis. Only 3 questions (state of gum health, loose teeth, tooth appearance) were found to be useful and valid in predicting serious periodontitis for this study population. Gum surgery, scaling and root planing were less frequently reported due to inaccessibility of most of the participants to regular dental visits as most belonged to lower socio-economic status.
Limitations and Recommendations
The performance of these variables in different racial and ethnic groups were not explored due to the small number of participants. Although Filipino language was the main medium used to state the questions in this study, several other local dialects might be more applicable for other ethnic groups and in other hospital institutions in the country. The medical institution where this study was conducted only represented the local tertiary government hospital in an urban setting acting as an end referral center for difficult cases of diabetes. Considering the different overall profile of target Filipino participants, a scoring system based on this local validation study of predictive factors would be better suited to screen candidate patients in need for immediate dental evaluation. Further studies using the recommended questions and proposed scoring will be needed to validate the questionnaire as a screening tool and to determine the cut off score that would be highly sensitive and specific in predicting presence of serious periodontitis among diabetic patients consulting a physician.
Statement of AuthorshipAll authors have given approval to the final version submitted.
Author DisclosureAll the authors declared no conflicts of interest.
Funding SourceNone.
1. Zimmet P, Alberti KGMM, Shaw J. Global and societal implications of the diabetes epidemic. Nature. 2001;414:782-7. http://dx.doi.org/10.1038/414782a.
2. Global status report on noncommunicable diseases 2014. Geneva, World Health Organization, 2012. 3. Shaw JE, Sicree RA, Zimmet PZ. Global estimates of the prevalence of diabetes for 2010 and 2030. Diabetes Res Clin Pract. 2010;87(1):4-14. http://dx.doi.org/10.1016/j.diabres.2009.10.007. 4. Soria MLB, Sy RG, Vega BS, Ty-Willing T, Abenir-Gallardo A, Velandria F, et al. The incidence of type 2 diabetes mellitus in the Philippines: A 9-year cohort study. Diabetes Res Clin Pract. 2009;86(2):130-3. http://dx.doi.org/10.1016/j.diabres.2009.07.014. 5. Chaudhari M, Hubbard R, Reid RJ, Inge R, Newton KM, Spangler L, et al. Evaluating components of dental care utilization among adults with diabetes and matched controls via hurdle models. BMC Oral Health. 2012;12:20. http://dx.doi.org/10.1186/1472-6831-12-20. 6. Yuen HK, Onicescu G, Hill EG, Jenkins C. A survey of oral health education provided by certified diabetes educators. Diabetes Res Clin Pract. 2010;88(1):48-55. http://dx.doi.org/10.1016/j.diabres.2009.12.015. 7. Newton KM, Chaudhari M, Barlow WE, Inge RE, Theis MK, Spangler LA, et al. A population-based study of periodontal care among those with or without diabetes. J Periodontol. 2011;82(12):1650-6. http://dx.doi.org/10.1902/jop.2011.100609. 8. Daniel R, Gokulanathan S, Shanmugasundaram N, Lakshmigandhan M, Kavin T. Diabetes and periodontal disease. J Pharm Bioallied Sci. 2012;4(6):280-2. http://dx.doi.org/10.4103/0975-7406.100251. 9. Löe H. Periodontal disease: The sixth complication of diabetes mellitus. Diabetes Care. 1993;16(1):324-34. http://dx.doi.org/10.2337/diacare.16.1.329. 10. The pathogenesis of periodontal diseases. J Periodontol. 1999;70(4):457-70. 11. Mealey BL, Oates TW. Diabetes mellitus and periodontal diseases. J Periodont. 2006;77(8):1289-1303. http://dx.doi.org/10.1902/jop.2006.050459. 12. Glavind L, Lund G, Löe H. The relationship between periodontal state and diabetes duration, insulin dosage and retinal changes. J Periodontol. 1968;39(6):341-7. http://dx.doi.org/10.1902/jop.1968.39.6.341. 13. Apoorva SM, Sridhar N, Suchetha A. Prevalence and severity of periodontal disease in type 2 diabetes mellitus (non-insulin-dependent diabetes mellitus) patients in Bangalore city: An epidemiological study. J Indian Soc Periodontol. 2013;17(1):25-9. http://dx.doi.org/10.4103/0972-124X.107470. 14. Bharateesh JV, Ahmed M, Kokila G. Diabetes and oral health: A case-control study. Int J Prev Med. 2012;3(11):806-9. 15. Weinspach K, Staunfenbiel I, Memenga-Nicksch S, Ernst S, Geurtsen W, Günay H. Level of information about the relationship between diabetes mellitus and periodontitis- Results from a nationwide diabetes information program. Eur J Med Res. 2013;18:6. 16. Bitong E, Jasul GV, Dellosa MAG. Prevalence of periodontitis and its association with glycemic control among patients with type 2 diabetes mellitus seen at St.Luke's Medical Center. Philipp J Int Med. 2010;48(1):9-14. 17. Lee IC, Shieh TY, Yang YH, Tsai CC, Wang KH. Individuals' perception of oral health and its impact on the health-related quality of life. J Oral Rehabil 2007;34(2):79-87. http://dx.doi.org/10.1111/j.1365-2842.2006.01694.x. 18. Sandberg GE, Wikblad KF. Oral health and health-related quality of life in type 2 diabetic patients and non-diabetic controls. Acta Odontol Scand. 2003;61:141-8. 19. Teeuw WJ, Gerdes VEA, Loos BG. Effect of periodontal treatment on glycemic control of diabetic patients. Diabetes Care. 2010;33(2):421-7. http://dx.doi.org/10.2337/dc09-1378. 20. Tomar SL, Lester A. Dental and other health care visits among U.S. adults with diabetes. Diabetes Care. 2000;23(10):1505-10. http://dx.doi.org/10.2337/diacare.23.10.1505. 21. Ofilada EJ ,Jimeno CA. A Survey on the barriers to dental care among individuals with type 1 diabetes mellitus. Ongoing publication. 2013. 22. O'Connor PJ, Desai J, Rush WA, Cherney LM, Solberg LI, Bishop DB. Is having a regular provider of diabetes care related to intensity of care and glycemic control? J Fam Prac. 1998;47(4):290-7. 23. IDF Clinical Guideline Taskforce. IDF guideline on oral health for people with diabetes. Brussels: International Diabetes Federation, 2009. 24. Jimeno CA. Updates on the UNITE for Diabetes Philippine Practice Clinical Practice Guidelines for Diabetes Part 2. PPD Compendium of Philippine Medicine, 2014. 25. Eke PI, Genco RJ. CDC periodontal disease surveillance project: Background, objective, and progress report. J Periodontol. 2007;78(7s):1366-71. http://dx.doi.org/10.1902/jop.2007.070134. 26. Miller K, Eke PI, Schoua-Glusberg A. Cognitive evaluation of self-report questions for surveillance of periodontitis. J Periodontol. 2007;78(7s):1455-62. http://dx.doi.org/10.1902/jop.2007.060384. 27. Slade G. Interim analysis of validity of periodontitis screening questions in the Australian population. J Periodontol. 2007;78(7s):1463-70. http://dx.doi.org/10.1902/jop.2007.060344. 28. Eke PI, Dye B. Assessment of self-report measures for predicting population prevalence of periodontitis. J Periodontol 2009;80(9):1371-9. http://dx.doi.org/10.1902/jop.2009.080607. 29. American Diabetes Association. Standards of medical care in diabetes- 2013. Diabetes Care. 2013;36(1):S11-S66. http://dx.doi.org/10.2337/dc13-S011. 30. Dye BA, Barker LK, Selwitz RH, Lewis BG, Wu T, Fryar CG, et al. Overview and quality assurance for the National Health and Nutrition Examination Survey (NHANES) oral health component, 1999-2002. Community Dent Oral Epidemiol. 2007;35(2):140-51. http://dx.doi.org/10.1111/j.1600-0528.2007.00310.x. 31. Tomar SL, Asma S. Smoking-attributable periodontitis in the United States: Findings from NHANES III. J Periodontol. 2000;71(5):74351. http://dx.doi.org/10.1902/jop.2000.71.5.743. 32. Albandar JM, Brunelle JA, Kingman A. Destructive periodontal disease in adults 30 years of age and older in the United States, 1988-1994. J Periodontol. 1999;70(1):13-29. http://dx.doi.org/10.1902/jop.1999.70.1.13. 33. Swets JA. Measuring the accuracy of diagnostic systems. Science. 1988;240(4857):1285-93. http://dx.doi.org/10.1126/science.3287615. 34. Nelson DE, Holtzman D, Bolen J, Stanwyck CA, Mack KA. Reliability and validity of measures from the Behavioral Risk Factor Surveillance System (BRFSS). Soz Praventivmed. 2001;46 (1):S3- S42.Authors are required to accomplish, sign and submit scanned copies of the JAFES Author Form consisting of: (1) the Authorship Certification that the manuscript has been read and approved by all authors, and that the requirements for authorship have been met by each author, (2) the Author Declaration that the article represents original material that is not being considered for publication or has not been published or accepted for publication elsewhere, (3) the Statement of Copyright Transfer [accepted manuscripts become the permanent property of the JAFES and are licensed with an Attribution-Share Alike-Non-Commercial Creative Commons License. Articles may be shared and adapted for non-commercial purposes as long as they are properly cited], (4) the Statement of Disclosure that there are no financial or other relationships that might lead to a conflict of interest. For Original Articles involving human participants, authors are required to submit a scanned copy of the Ethics Review Approval of their research. For manuscripts reporting data from studies involving animals, authors are required to submit a scanned copy of the Institutional Animal Care and Use Committee approval. For Case Reports or Series, and Images in Endocrinology, consent forms, are required for the publication of information about patients; otherwise, authors declared that all means have been exhausted for securing such consent. Articles and any other material published in the JAFES represent the work of the author(s) and should not be construed to reflect the opinions of the Editors or the Publisher.