Myanmar Clinical Practice Guideline for Osteoporosis
Tint Swe Latt1, Than Than Aye2, Ko Ko2, Thein Myint2, Ni Ni Hlaing2, Myint Thaung3 and Tet Tun Chit4
Prof. Tint Swe Latt
President, Myanmar Society of Endocrinology and Metabolism
University of Medicine 2, Yangon, Myanmar
Tel. No.: 959- 5167332
E-mail: proftsl@gmail.com
e-ISSN 2308-118x
Printed in the Philippines
Copyright © 2012 by the JAFES
Received October 19, 2012. Accepted October 29, 2012
Osteoporosis is a disease in which the density and quality of bone are reduced, leading to weakness of the skeleton and increased risk of fracture, particularly of the spine, wrist and hip.
Generally, osteoporosis in Myanmar is still a neglected disease entity in the national priority health problems. Due to the low level of awareness on osteoporosis and its consequent fragility fractures, limited availability and accessibility of standard diagnostic tools and medications, osteoporosis is mainly under diagnosed and under-treated in daily clinical practice. It is not mentioned in the prioritized diseases in the national health plan.
Osteoporosis and associated fractures are an important cause of mortality and morbidity.
Osteoporosis is a global problem, which is increasing in significance as the population of the world both grows and ages. Worldwide, lifetime risk for osteoporotic fractures in women is 30-50%. In men risk is 15-30%.
Currently, the prevalence of osteoporosis in Myanmar is unknown due to lack of proper diagnostic facilities. The only data available are from two studies done in Yangon and Mandalay by using calcaneal ultrasound. However, the reference values of bone mineral density was from Caucacians e, the ultrasound diagnostic method was not standardized and the data from these studies cannot estimate the real prevalence of osteoporosis in Myanmar’s population.
Over the last decade, there has been a paradigm shift in the prevention and treatment of osteoporosis. The focus now is on preventing fragility fractures and their negative consequences, rather than on treating low Bone Mineral Density (BMD), which is viewed as only one of several risk factors for fracture. There are several clinical factors which can increase the risk of fracture, and therefore, it is important to take an integrated approach and to base treatment decisions on the absolute risk of fracture. There is a gap in the care of high-risk patients, as many patients with fractures do not undergo appropriate assessment or treatment. The Myanmar CPG on osteoporosis focuses on the assessment and management of post menopausal women and men over age 50 who are at high risk of fragility fractures and the integration of new tools for assessing the 10-year risk of fracture into overall management.
To develop Myanmar Clinical Practice Guideline(CPG) for health care providers that focus on prevention, diagnosis, and treatment aspects of osteoporosis and osteoporosis related fragility fractures among postmenopausal women and men over the age of 50.
(1) To develop guidelines on healthy lifestyle (namely nutrition and physical activity) for the prevention of osteoporosis in Myanmar context.
(2) To formulate cost effective ways to diagnose osteoporosis using bone densitometry technique, Osteoporosis Screening Tool for Asians (OSTA), spine radiographs, 10-year fracture risk assessment (FRAX) tool.
(3) To formulate evidence-based recommendations on the pharmacologic management of osteoporosis
(4) To develop the assessment plan for fragility fracture(s)
(5) To develop recommendations for the management of fragility fracture(s)
Methodology for the development of Myanmar CPG for Osteoporosis
The Guidelines Committee was formed among the members of the Special Interest Group on Osteoporosis.
First of all, rounds of discussion were held among physicians, endocrinologists, orthopedic surgeons, gynecologists, radiologists, rheumatologists, physiatrists, general practitioners and allied health professionals to ascertain their view on osteoporosis and to identify priorities for the Myanmar CPG on osteoporosis.Reviews of the literature were made according to these priorities to collect updated knowledge on diagnosis, prevention and treatment for osteoporosis and fragility fracture. Special references were made on those guidelines with reliable methodology and relevant epidemiological background to Myanmar (Canada, American, Asian, Philippine, Australia, Strong bone Asia). The Guideline Committee developed clinical Practice Guideline on osteoporosis with particular emphasis on the issues raised by discussion with Myanmar Health Care Providers.
The draft of the Myanmar CPG on Osteoporosis was discussed among the relevant healthcare providers on 2012 World Osteoporosis Day and resulted in the final CPG on osteoporosis.
1. Exercise
(a) For those with or at risk for osteoporosis: appropriate resistance training and/or weight-bearing aerobic exercise.
(b) For those with vertebral fractures: directed core stability exercises.
(c) For those at risk of falls: exercises that focus on balance (e.g., Tai chi, balance and/or gait training).
(d) For those in long-term care at high risk: use of hip protectors.
2. Smoking: Avoidance of tobacco usage is recommended
3. Alcohol: Avoidance of excessive consumption of alcohol is recommended (< 3 units per day in men and <2 units per day in women)
4. Exercises: daily exercise of 20 – 30 minutes for 3 – 5 times a week such as regular walking, jogging, aerobic dancing and tai-Chi or Chi-gong
Calcium: 600–1200 mg oral daily should be prescribed.
Vitamin D:
For healthy adults at low risk of vitamin D deficiency, routine supplementation with 400–1000 IU (10–25 mg) vitamin D3 daily is recommended.
For adults over age 50 at moderate risk of vitamin D deficiency, supplementation with 800–1000 IU (20–25 mg) vitamin D3 daily is recommended.
Osteoporosis Screening Tool for Asians (OSTA) is recommended to identify the individual's risk for Osteoporosis where central dual x-ray absorptiometry (DXA) is unavailable.
Click here to download Figure 1
Figure 1. Osteoporosis self-assessment tool for Asians (OSTA)
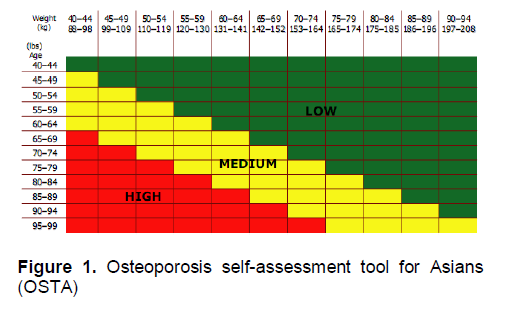
· High risk patients: to measure BMD, if possible, and consider drug treatment even if BMD is not available.
· Medium risk patients: to measure BMD and consider drug treatment if BMD is low.
Low risk patients: not to measure BMD unless other risk factors are present. Fracture Risk Assessment Tool (FRAX) tool should be used for all postmenopausal women with at least one WHO risk factor.
It is recommended that diagnosis of osteoporosis be based on WHO diagnostic classification criteria for bone mass using the Dual Energy X-ray Absorptiometry (DEXA) as the gold standard.
According to the World Health Organization criteria, osteoporosis is diagnosed by bone mineral density (BMD) measurements.
Normal bone density: T-score greater than -1
Osteopenia (low bone mass): T-score between -1 and -2.5
Osteoporosis: T-score lower than -2.5
(Note: The T-score is the number of standard deviations of BMD below the young normal mean).
DEXA is currently the ‘gold standard’ for the diagnosis of osteoporosis. BMD can be measured at the hip, the lumbar spine and the total body.
Ultrasound measurements are not recommended for diagnosing osteoporosis.
The OSTA is applicable in Myanmar as the resources for DEXA are constrained.
1. DEXA measurements should be performed on the following subjects:
1. Postmenopausal women 65 years or older, regardless of additional risk factors.
This recommendation includes women 65 years or older, who have been taking osteoporosis therapy and who have not had a BMD test.
2. Postmenopausal women younger than 65 years and with 1 or more of the following additional risk factors for osteoporosis:
• Parental history of hip fracture;
• Current cigarette smoking;
• A body weight less than 57.2 kg for Caucasians; for Asian populations, a criteria of BMI <19
• Use of (or plans to use) oral corticosteroids at 7.5mg/day for longer than 3 months;
• Serious long-term conditions thought to increase fracture risk, such as hyperthyroidism or malabsorption.
Postmenopausal women who have had a fracture of any type as an adult after age 45 years
2. Biochemical markers of bone turnover
Biochemical markers of bone turnover can be used for assessing adherence to, effectiveness of therapy and assessment of fracture risk if available.
The following biochemical markers of bone turnover can be measured in serum and urine:
Biochemical markers of bone formation (in serum)
• Procollagen type I propeptides (PINP)
Biochemical markers of bone resorption
• C and N-telopeptides of type I collagen cross-link (in serum and urine)
3. Other Tests
The following are the routine investigations that should be performed in patients with osteoporosis: complete blood count and erythrocyte sedimentation rate, renal function tests, liver function tests, general biochemistry including serum calcium, phosphate, and alkaline phosphatase, thyroid function tests, testosterone level in men.
Other special tests such as serum protein electrophoresis, parathyroid hormone and 25-hydroxy vitamin D are only indicated if the initial work-up is suggestive of a related disorder.
Among those with BMD examination treatment should be started if:
a. Vertebral compression fracture/s confirmed through radiograph (clinical osteoporosis);
b. BMD T-score of ≤ -2.5;
c. BMD T-score between - 1 and - 2.5 SD with any of the following:
c.1. History of previous fracture
c.2. Secondary causes associated with high risk for fracture
c.3. 10-year probability of hip fracture ≥ 3% or any major osteoporosis related fracture of ≥20% based on the FRAX estimates
Among those without BMD measurement, it is suggested that treatment be started if patient:
(i) belongs to the high risk category based on OSTA tool where central BMD cannot be done or not available
(ii) has a 10-year probability of hip fracture ≥ 3% or any major osteoporosis related fracture of ≥ 20% based on the FRAX estimates
Recommended pharmacologic options
i. Alendronate is the first line option for all osteoporosis. The recommended dose is 70 mg once weekly or 10 mg daily for 5 years. It should be used with caution in renal impairment and history of oesophageal reflux/hiatus hernia. These agents should be taken on an empty stomach at least 30 minutes before breakfast.
ii. Zoledronicacid is recommended as a second line for those who have GI intolerance to oral bisphosphates. Recommended dosage is 5 mg IV infused over at least 15minutes every 12 months.
iii. Raloxifene, selective estrogen receptor modulators (SERM) is recommended as 3rd line of medical treatment. It is effective for prevention and treatment of vertebral fracture in post-menopausal women. Prescribed dosage is 60 mg once daily. It has not been shown to decrease the risk of hip fractures, but reduces the risk of vertebral fractures.
iv. Strontium ranelate has been shown to both increase osteoblastic bone information and reduce osteoclastic bone resorption. Given at 2grams daily orally, it may be used as first line therapy in high risk patient or in those intolerant of bisphosphonates as a second line therapy. It is indicated in post-menopausal osteoporosis for reduction of fracture risk in hip and vertebrae.
v. Calcitonin spray 200IU daily in alternating nostrils can be recommended in the initial first month after an acute vertebral compression fracture. It is not recommended for long term treatment. It has no effect on prevention of hip fracture. It is less effective for increasing bone density than estrogen or bisphosphates.
vi. Teriparatide (1-34 parathormone) is not available locally and currently needs prescription by a specialist in bone disease or an endocrinologist. It can be recommended in those who suffer further fractures despite treatment with other agents.
vii. Estradiol is not recommended for treatment of osteoporosis.
It is reasonable to consider starting prophylactic therapy in patients on chronic steroids. Long term corticosteroid of ≥3 months at a prednisolone-equivalent dose ≥7.5 mg daily.
Alendronate is recommended for the treatment of steroid-induced osteoporosis.
• Measurement of BMD using DEXA is currently recommended for assessment of fracture risk in individuals treated with CS.
• Anti-resorptive therapy is recommended for subjects with a BMD T-score of -1.5 and in whom it is intended to continue therapy for at least 3 months; or subjects aged 65 years or over with a prior fragility fracture. Calcium and vitamin D supplementation are recommended for all CS patients.
The fracture during activity that would not normally injure young healthy bone (i.e., Fall from standing height or less) with trivial force usually accompanied with risk factors for osteoporosis or risk factors for fall or risk factors for fracture. (IOF)
• It is suggested that exercise be encouraged among both the housebound elderly and those in the community due to its benefit on balance and indirectly on fracture prevention.
• Other than exercise, provision of hip protectors can be considered to reduce incidence of hip fracture.
• It is recommended that high risk Postmenopausal Women (PMW) be given pharmacologic options (e.g., bisphosphonates, selective estrogen receptor modulator, hormonal replacement therapy, calcitonin, strontium ranelate to increase BMD or reduce fracture risks.)
The major risk factors for fragility fracture are prior fragility fracture; increasing age, low BMD, low body weight, family history of osteoporotic fracture, glucocorticoids use and current smoking.
There are three main assessment areas after fracture
(1) Bone morphology and bone mass density
(2) Patient’s underlying medical diseases
(3) Underlying etiology of osteoporosis and risk factors
DEXA is not practicable immediately after getting fragility fracture.
X-ray observation- osteopenia on x-ray implies significant bone loss with decreased opacity, thin cortices, wide canals, current fractures, healing fractures.
DEXA— current gold standard for BMD
Fragility fracture patient assessment in addition to routine pre-op or fracture evaluation :-
Thorough history taking and physical examination relevant to fragility fracture should be done.
Laboratory tests are recommended for assessment to exclude secondary osteoporosis
Policy for osteoporotic fracture management: immediate hospitalization whenever feasible. The following objectives should be followed:
(1) Immediate comfort with pain relief and protection
(2) Setup the appropriate specific fracture care
(3) Minimize dependences and maximize the mobility
(4) Treat underlying osteoporosis and monitor
(5) Identification and prevention of risk factors
(6) Patient’s education
Monitoring Plan after fracture fixation
• Fracture stability follow up every three weeks
• Fracture union follow up at every six weeks
• Counseling for risk reduction immediately after discharge and at follow-up
This is the first published guideline that focused on both medical and surgical aspect of osteoporosis and fragility fracture. It is advisable for all stakeholders to use the guideline so as to be able to give optimal health care for individual afflicted with the condition. This guideline is meant to help clinicians to make appropriate decision in management of osteoporosis and its consequent fragility fracture. However, clinician's best clinical judgments are the most important assets in the management of these patients. Regular review of these guidelines will be made in the light of fresh and new evidence, which will come up in the medical literature in future.
1. Aasis Unnanuntana, Brian P. Gladnick, Eve Donnely. Joseph M. Lane. Current Concept review: The assessment of Fracture risk; J Bone Joint Surg Am. 2010;92:743-53
2. Apley, AG, (2010), Apley's System of Orthopaedics and Fracture, 9th ED. P131-135. New York: Hodder Arnold
3. Barrett-Connor E, Mosca L, Collins P, et al; Raloxifene Use for The Heart (RUTH) Trial Investigators.
4. Bischoff-Ferrari HA, Willett WC, Wong JB, Giovannucii E, Dietrich T, Dawson-Hughes B. Fracture prevention with vitamin D supplementation: A meta-analysis of randomized controlled trials. JAMA.2005;293:2257–2264.
5. Black DM, Delmas PD, Eastell R, et al. Once-yearly zolendronic acid for treatment of postmenopausal osteoporosis. N Engl J Med. 2007; 356:180–1822.
6. Black DM, Schwartz AV, Ensrud KE, et al. Effects of continuing or stopping alendronate after 5 years of treatment. JAMA.2006;296:2927–2938.
7. Chesnut CH, Silverman S, Andriano K, et al, for the PROOF Study Group. A randomized trial of nasal spray salmon calcitonin in postmenopausal women with established osteoporosis: The Prevent Recurrence of Osteoporotic Fractures Study. Am J Med. 2000;109:267–276.
8. Clinical guideline for the prevention and treatment of osteoporosis in postmenopausal women and older men. The Royal Australian College of General Practitioners, February 2010.
9. Consensus Development Conference: prophylaxis and treatment of osteoporosis. American Journal of Medicine: 1991:90:107-10
10. Cranney A, Tugwell P, Adachi J, et al. Meta-analysis of risedronate for the treatment of postmenopausal osteoporosis. Endocr Rev. 2002;23:517–523.
11. Cranney A, Tugwell P, Zytaruk N, et al. Meta-analysis of calcitonin for the treatment of postmenopausal osteoporosis. Endocr Rev. 2002;23:540–551.
12. Cranney A, Wells G, Willan A, et al. Meta-analysis of alendronate for the treatment of postmenopausal osteoporosis. Endocr Rev. 2002;23:508–516.
13. Effects of raloxifene on cardiovascular events and breast cancer in postmenopausal women. N Engl J Med. 2006; 335:125–137.
14. Fujiwara S, Nakamura T, Orimo T.H, Hosoi I, Gorai I, Oden H.A, Johansson H, Kanis J.A Development and application of a Japnes model of the WHO Fracture Risk assessment tool (FRAX TM): Osteoporosis Int (2008) 19:429-435
15. Genant HK, Engelke K, Fuerst T, Gluer CC, Grampp S, Harris ST, Jergas M, Lang T, Lu Y, Majumdar S, Mathur A, Takada M. Non-invasive assessment of bone mineral and structure: State of the art, JBone Miner Res, 19996;11:707-730
16. Health in Myanmar 2012
17. Health in Myanmar Statistics 2011
18. Johansson H, Kanis J. A, Oden A, Johnnell O, McCloskey E. BMD, clinical risk factors and their combination for hip fracture prevention.
19. Lau EMC, SambrookP,SeemanE,Leong KH, Leung PC and Delmas P. Guidelines for diagnosing, prevention and treatment of osteoporosis in Asia. APLAR Journal of Rheumatology 2006; 9: 24–36.
20. Li-Yu J, Perez EC, Canete A, Bonifacio L, Llamado LQ, Martinez R, Lanzon A and Sison M. Consensus statements on osteoporosis diagnosis, prevention, and management in the Philippines. International Journal of Rheumatic Diseases 2011; 14: 223–238.
21. Myanmar Medical Association, Special Interest Group on Osteoporosis. Unpublished data on prevalence of osteoporosis in Yangon, Myanmar, 2009.
22. National Institute of Health (United States) Consensus conference, 2000
23. National Osteoporosis Foundation. Clinician’s Guide to Prevention and Treatment of Osteoporosis. Washington, DC: National Osteoporosis Foundation; 2010.
24. NICE guidelines for Alendronate, etidronate, risedronate, raloxifene, strontium ranelate and teriparatide for the secondary prevention of osteoporotic fragility fractures in postmenopausal women (amended). www.nice.org.uk/guidance/TA161
25. NICE guidelines for Alendronate, etidronate, risedronate, raloxifene, strontium ranelate and teriparatide for the secondary prevention of osteoporotic fragility fractures in postmenopausal women (amended). www.nice.org.uk/guidance/TA16
26. Ostoeporosis Guideline of Malaysia, Thailand, USA
27. Osteoporosis Screening, Diagnosis and Treatment Guideline in United States: https//www.ghc.org/all-sites/guidelines/osteoporosis.pdf
28. Papaioannou A, Morin S, Cheung AM, et al. 2010 clinical practice guidelines for the diagnosis and management of osteoporosis in Canada: Summary CMAJ2010; 182(17):1864-1873.
29. Park-Wyllie LY, Mamdani MM, Juurlink DN, et al. Bisphosphonate use and the risk of subtrochanteric or femoral shaft fractures in older women. JAMA . 2011;305:783–789
30. Performance of Osteoporosis Self-assess DAJ Muslim, EF Mohd, AY Sallehudin, TMS TengkuMuzaffar,AM Ezane, MMED Radment Tool for Asian (OSTA) for Primary Osteoporosis in Post-menopausal Malay Wome, Malaysian Orthopaedic Journal 2012 Vol 6 No 1
31. Summary Meeting Report, Brussels, Belgium, 5-7 May 2004.
32. WHO scientific group on the assessment of osteoporosis at primary health care level
33. WHO (1994) Assessment of Fracture risk and its application to screening for post menopausal osteoporosis (WHO technical report series, No. 843)
34. WHO (2003) Prevention and management of osteoporosis ( WHO technical report series, No. 921)
Authors are required to accomplish, sign and submit scanned copies of the JAFES Declaration that the article represents original material that is not being considered for publication or has not been published or accepted for publication elsewhere.
Consent forms, as appropriate, have been secured for the publication of information about patients; otherwise, authors declared that all means have been exhausted for securing such consent.
The authors have signed disclosures that there are no financial or other relationships that might lead to a conflict of interest. All authors are required to submit Authorship Certifications that the manuscript has been read and approved by all authors, and that the requirements for authorship have been met by each author.