In his publications from 1938 to 1968, Sheehan elegantly described the natural history, clinical signs and pathologic findings of the syndrome that results from postpartum necrosis of the anterior lobe of the pituitary gland. The exact pathogenesis of the disease is not well understood, since many women who suffer severe hemorrhage at delivery apparently escape damage to the anterior pituitary.[1]-[3] Many of the cases remain undetected until years later, when hypothyroidism or secondary adrenal insufficiency become evident in a woman who had postpartum hemorrhage.[4]
A recent epidemiologic study from the Kashmir Valley of the Indian subcontinent estimated the prevalence of SS to be about 3% for women above 20 years of age, almost twothirds of whom had home deliveries. However, SS is a rare cause of hypopituitarism in developed countries. In a study of 1,034 adults with hypopituitarism, SS was the sixth most frequent cause of growth hormone (GH) deficiency, being responsible for 3.1% of cases.[5] In a retrospective nationwide analysis in Iceland, the prevalence of SS in 2009 was estimated to be 5.1 per 100,000 women.[6] The clinical presentation of Sheehan’s syndrome varies from nonspecific manifestations such as weakness, anemia and fatigue, to severe pituitary dysfunction resulting to coma and even death. A medical history of postpartum hemorrhage, failure to lactate and cessation of menses are helpful clues to the diagnosis.[7]-[10]
Sheehan’s syndrome that initially presents with hyponatremia and hypoglycemia is rarely reported in literature.[11] Hypothyroidism and glucocorticoid deficiency decrease free water clearance independent of vasopressin and subsequently cause hyponatremia. The syndrome of inappropriate antidiuretic hormone secretion (SIADH) and volume depletion are other factors that also lead to hyponatremia.[12][13] Recurrent hypoglycemia due to growth hormone, adrenal and other counter-regulatory hormone deficiencies is a less known complication of SS.[14] In this study, we present a case of Sheehan’s syndrome with hyponatremia and hypoglycemia that improved after replacement with glucocorticoids.
CASEA 47-year old Indonesian housewife was admitted to our hospital in December 2013 due to sudden loss of consciousness (Figure 1). She was found to have recurrent episodes of loss of consciousness in the last 6 months, accompanied by symptoms of generalized fatigue, weakness and anorexia. She noticed dry skin and thinning of hair starting 3 years ago. She had no history of fever, headache, vomiting, seizure, head injury or loose stools. She was multigravid (G7P6), with her last baby delivered at home by a midwife at the age of 33 years. She had severe postpartum hemorrhage necessitating hospitalization and transfusion with six units of blood. After the eventful delivery, she was unable to produce breastmilk and subsequently had irregular menstrual cycles in the last 14 years. She had been amenorrheic for one year.
Click here to download Figure 1Figure 1. Image of patient at presentation with sudden loss of consciousness.

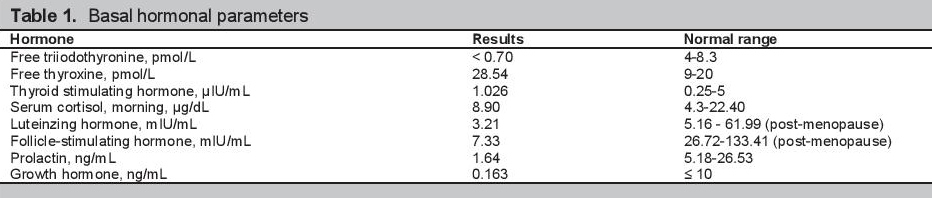
On physical examination, the patient appeared chronically ill with depressed sensorium (Glasgow coma scale E3V3M5). She was afebrile, with stable vital signs (pulse rate 72 beats/min, regular; blood pressure 100/70; respiratory rate 20 cycles/min). She had dry, rough and cold skin, with good turgor. She had pale palpebral conjunctivae and absent axillary and pubic hairs. Laboratory tests revealed normocytic, normochromic anemia with low hemoglobin concentration (7.8 g/dL). She had hyponatremia (109 mmol/L) and hypoglycemia (40 mg/dL), normal potassium (3.9 mEq/L) and creatinine (0.6 mg/dL), top normal urea (20 mg/dL) and low serum osmolality (233 mOsm/kg). Arterial blood gas analysis revealed pH 7.424, PO2 146.9 mmHg and PCO2 24.9 mmHg. Urine electrolytes showed natriuresis (urinary sodium 273 mmol/24 hours, normal value 40-220 mmol/24 hours) and normal potassium excretion (urinary potassium 20.3 mmol/24 hours, normal value 15-125 mmol/24 hours). Basal hormonal workup showed low levels of growth hormone (GH), prolactin (PRL), luteinizing hormone (LH) and follicle stimulating hormone (FSH); and normal cortisol. She also had low free triiodothyronine (FT3) and normal thyroid stimulating hormone (TSH) (Table 1). Magnetic resonance imaging (MRI) of the brain showed an empty sella appearance, with the small-volume pituitary gland flattened against the sellar floor (Figure 2). These findings confirmed the diagnosis of Sheehan's syndrome.
Click here to download Table 1Table 1. Basal hormonal parameters
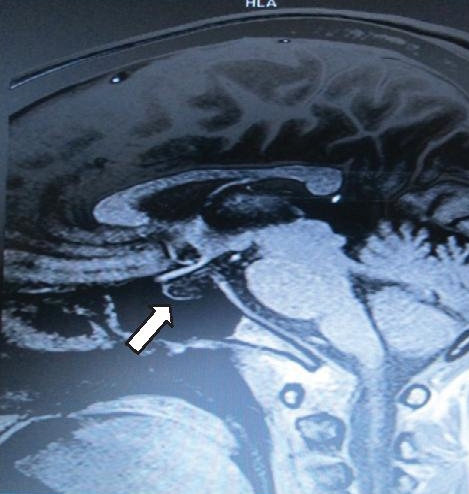
Click here to download Figure 2
Figure 2. Sagittal enhanced T1-weighted magnetic resonance image showing empty sella appearance, with the pituitary gland flattened against the sellar floor.
Following the clinical and laboratory findings, she was given saline infusion and glucocorticoid replacement with intravenous methylprednisolone at 125 mg/day for 3 days. There was improvement of hypoglycemia, hyponatremia and clinical symptoms. She was managed with oral steroids subsequently.
Sheehan’s syndrome is characterized by pituitary necrosis after severe postpartum hemorrhage and hypovolemia. Vasospasm, thrombosis and vascular compression of the hypophyseal arteries have also been described as possible causes of the syndrome. Enlargement of the pituitary gland, small sellar size, disseminated intravascular coagulation and autoimmunity have been suggested to play a role in the pathogenesis of SS. The syndrome is characterized by varying degrees of anterior pituitary dysfunction. It may cause hypopituitarism either immediately or after a delay of several years, depending on the degree of tissue destruction. Some degree of hypopituitarism occurs in nearly one-third of patients with severe postpartum hemorrhage. Although symptomatic posterior pituitary dysfunction is uncommon, many patients have impaired neurohypophyseal function tests.[5][16][17]
Forty years ago, it was estimated that the prevalence of Sheehan’s syndrome was about 100 to 200 per 1,000,000 women.5 It is now considered a very rare obstetric complication. The clinical presentation of Sheehan’s syndrome ranges from long-standing non-specific features such as weakness, fatigue and anemia, to profound abrupt hypopituitarism resulting in coma and death.[18]
A retrospective study of 20 patients with SS, which included patients aged 28 to 71 years, showed that the interval between the beginning of the disease and the definitive diagnosis varied between 5 to 25 years. All of the patients had a history of a serious bleeding during or after delivery. Six patients had received blood transfusion for severe bleeding. All of the patients described inability to nurse and subsequent failure of menstrual cycles to return to normal patterns.[2] Sunil and colleagues reported that failure to resume menstruation and agalactia were the most common symptoms, found in 100% and 72% of the patients, respectively.[19] Sert and colleagues reported that 9 of their 28 patients presented with disturbance in consciousness.[3] In the report by Ozkan and colleagues, they found 3 patients referred to the emergency service for hypoglycemia, 3 for hypothyroidism and one for hyponatremia.[2] Our patient experienced altered consciousness associated with weakness beginning 6 months before admission. A detailed obstetric history revealed severe hemorrhage following delivery of her seventh pregnancy, with ensuing failure to produce breast milk and irregular menstrual cycles.
As a presenting manifestation of Sheehan’s syndrome, severe hyponatremia causing altered sensorium has rarely been described in the literature. This is probably due to the slow evolution of the disease into its chronic form.[14] Punwell and colleagues found mild to severe hyponatremia in 9 of 13 patients with Sheehan’s syndrome.[20] The cause of hyponatremia in Sheehan’s syndrome is still open to debate. Cases of severe hyponatremia, with serum sodium levels below 125 mmol/L, developing 16 years after postpartum bleeding have been reported. Adrenal insufficiency is one of the most likely causes of hyponatremia in SS. SIADH may also be responsible for hyponatremia in patients with Sheehan’s syndrome.[21][22] Inappropriate secretion of antidiuretic hormone is known to occur in states of adrenocorticotropin deficiency. The mechanism by which hypopituitarism leads to decreased sodium concentration is complex and only partially understood. There is evidence of water retention as a result of inappropriately high levels of vasopressin. Animal experiments and clinical observations suggest that glucocorticoids tonically inhibit the secretion of vasopressin. A sudden loss or decrease in the inhibitory control may lead to rapid serum elevations of vasopressin. Another potential mechanism for the elevation in vasopressin is the uncontrolled release of the hormone from the posterior hypophysis in the setting of ischemia.[23] In our patient’s case, we found severe hypoosmolar hyponatremia with normovolemia, and increased urinary sodium. Low serum osmolality and elevated urine osmolality suggested SIADH.
Hypoglycemia in a case of hypopituitarism is more often seen in pituitary apoplexy than Sheehan's syndrome. Endocrine deficiency is the next most common cause of hypoglycemia (20%), second only to diabetes treatments (42%). Of these deficiencies, hypopituitarism is the leading cause, with Sheehan’s syndrome being the most common underlying etiology (44%).[15] In a case review conducted by Ozkan and Colak, 3 out of 20 Sheehan’s syndrome patients (15%) presented with hypoglycemia.[2] Cortisol deficiency results in glycogen depletion by causing anorexia and weight loss. This increases reliance on the gluconeogenesis pathway. Glycogen depletion and low levels of gluconeogenetic precursors due to cortisol deficiency result to an impaired ability to tolerate fasting. Growth hormone deficiency also contributes to hypoglycemia. In some cases where there is only partial pituitary necrosis, the syndrome can present in an atypical and incomplete manner, further complicating the diagnosis.[24] Our patient presented with low blood glucose during hospitalization prior to the diagnosis of Sheehan’s syndrome. Hormonal studies showed decreased growth hormone and normal cortisol.
Murat and colleagues reported that the pattern of hormone deficiency in Sheehan’s syndrome is variable. Hormone deficiencies following ischemic infarction of pituitary include GH (88%), gonadotropin (58 to 76%), and corticotropin (66%). Secondary hypothyroidism occurs was found in 42 to 53% of patients, and prolactin deficiency in 67 to 100% of patients.[3] In a review of 18 cases of SS at diagnosis, Sanval noted that lactotroph and gonadotroph failure were present in all patients, but corticotroph preservation was documented in 3 (16.7%) and thyrotroph in 2 (11.1%) patients. The anatomical location of GH and prolactin cells in the lower lateral region of the adenohypophysis make them most susceptible to ischemic damage.[25] In our patient’s case, we found low FT3 with normal TSH, supporting the diagnosis of central hypothyroidism. We also found low plasma levels of FSH, LH and prolactin.
The main radiologic finding of SS is the image of an empty sella (seen in 70% of patients) or partially empty sella (30%). The time-dependent evolution of the findings on MRI in SS has been observed to begin acutely with non-hemorrhagic changes in signal intensity consistent with central infarction, along with peripheral and heterogeneous central enhancement in an enlarged pituitary gland. The findings are consistent with patchy central ischemic necrosis in an enlarged gland and are followed by pituitary gland atrophy and an empty sella. These findings on MRI characterize SS and provide early confirmation of the clinical diagnosis.[26]-[28] In our patient, we found a widened sella turcica with a flattened pituitary gland consistent with an empty sella.
The treatment of Sheehan’s syndrome is replacement of the deficient hormones. ACTH and TSH deficiencies should be replaced with glucocorticoids and thyroxine respectively; mineralocorticoid replacement is usually not required.[18][29] Our patient improved clinically after methylprednisolone was given.
We encountered a rarely reported presentation of Sheehan’s syndrome, with documented hyponatremia and hypoglycemia in a patient with loss of consciousness. Her history of postpartum hemorrhage, failure to lactate and cessation of menses provided important clues to the diagnosis. Supported by hormonal studies and neuroimaging, we diagnosed the patient with SS and treated the patient appropriately. Some SS patients have been reported to have partial hypopituitarism, with preserved thyrotroph and corticotroph functions. Some are diagnosed late in the disease because the clinical features of SS are often subtle. Early diagnosis and appropriate treatment are necessary to reduce morbidity and mortality.
Ethical ConsiderationPatient consent has been procured prior to the case report study.
Statement of AuthorshipAll authors have given approval to the final version submitted.
Author DisclosureAll the authors have declared no conflict of interest to the work carried out in this paper.
Funding SourceNone.
[1] Haddock L. Sheehan’s syndrome in post-partum hemorrhage. In: A Textbook of Postpartum Hemorrhage: A Comprehensive Guide to Evaluation, Management and Surgical Intervention. CB Lynch, LG Keith, AB Lalonde, M Karoshi, eds. 1st ed. Dumfriesshire, UK: Sapiens Publishing, 2006.