Type 2 diabetes mellitus (T2DM) is the most common type of diabetes, contributing to more than 90% of diabetes mellitus cases worldwide.[1] The prevalence of diabetes mellitus in the Philippines according to the National Nutrition and Health Survey of 2008 is 7.2%.[2] The increasing prevalence of diabetes mellitus creates both medical and social problems due to the diabetic complications. If hyperglycemia, hypertension, dyslipidemia and obesity are appropriately addressed, prevention of these complications is possible. Physical activity, dietary modifications and behavioral therapy are part of the comprehensive treatment strategy in patients with T2DM.[3]
Regular exercise can offer both general health benefits and diabetes-specific health benefits. It can decrease the cardiovascular risk by improving lipid profile, lowering the blood pressure and inducing weight loss.[4] It also affects overall glycemic control through improved insulin sensitivity and lowered insulin requirements. All of these health benefits may have a great impact to decrease the risk for diabetes complications, reduce the progression of existing complications, and improve quality of life. Many metabolic adaptations occur in response to physical activity and these may lead to improvement of glycemic control for individuals with T2DM.[5]
Physical inactivity is one of the established risk factors that is responsible for about one-third of deaths due to diabetes.[6] Given the multiple health benefits that physical activity confers, the World Health Organization (WHO) recommends that all adults engage in moderate intensity physical activity for at least 150 minutes per week or vigorous-intensity physical activity for at least 75 minutes per week or an equivalent combination of moderate- and vigorous-intensity physical activity achieving at least 600 MET-minutes throughout a week, including activity for work, during transport and leisure time.
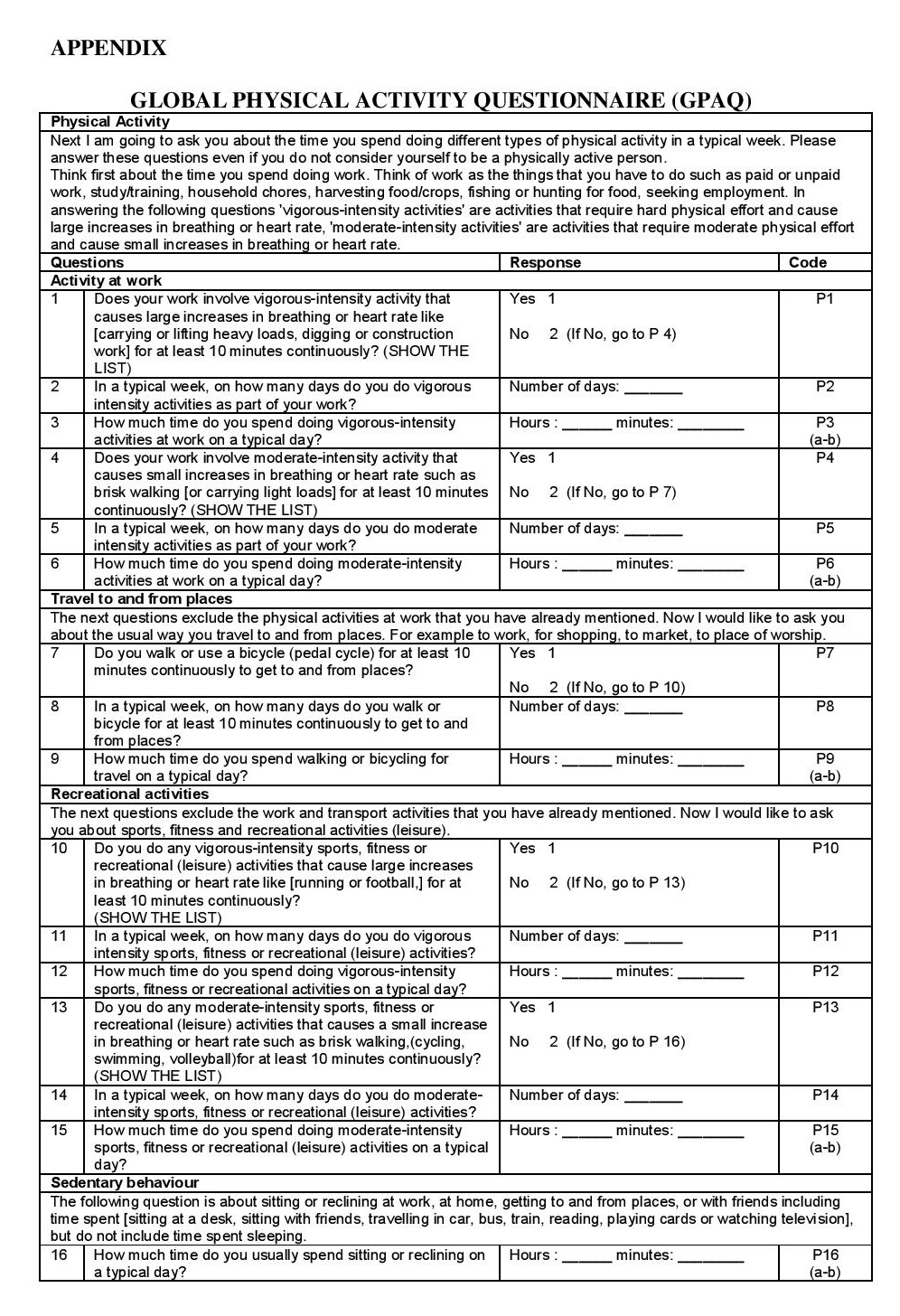
Physical activity level of patients with T2DM in this study was assessed using a WHO validated Global Physical Activity Questionnaire (GPAQ).[7] The GPAQ was selected above other physical activity tools because it provides summary of activities by recreation, occupation, and transportation domains. The questionnaire was used in the national nutrition survey and in a previous study with specific examples of local activities to help participants understand the questions in GPAQ; and a validity testing of self-administered GPAQ was conducted among non-diabetic Filipino adults.[8][9] A study among adult individuals of either gender aged 21 years and older was conducted to compare self-administered and original interviewer-administered versions of the GPAQ. For validity, GPAQ demonstrated fair-to-moderate correlations for moderate-to-vigorous physical activity (MVPA) for interviewer-administration (rs=0.46). Reliability for MVPA revealed moderate correlations (rs=0.63) for interviewer-administration.[10] Another study conducted to assess the test–retest reliability and concurrent validity of GPAQ against the other internationally acceptable physical activity questionnaire called International Physical Activity Questionnaire (IPAQ) and the criterion validity of the GPAQ instrument against objective measures like pedometer or accelerometer over 7 days which demonstrated reliability coefficients of moderate to substantial strength (Spearman’s rho 0.67 to 0.81; Kappa 0.67 to 0.73). Findings on concurrent validity between IPAQ and GPAQ also showed a moderate to strong positive relationship (range 0.45 to 0.65). The criterion validity were in the low-to-moderate correlations (range 0.06 to 0.35).[11]
Click here to download Appendix{kind=link}
Appendix.GLOBAL PHYSICAL ACTIVITY QUESTIONNAIRE (GPAQ)
Measuring levels of physical activity is an important initial step and a public health priority. However, currently, there is no available data on physical activity among Filipino patients with type 2 diabetes mellitus. Assessment for physical activity was only conducted among non-diabetic Filipino adults and school children. Thus, this study aims to assess the physical activity level among individuals with T2DM at Philippine General Hospital (PGH), Manila, Philippines using GPAQ. Other specific objectives are to describe the socio-demographic characteristics and health profiles of patients with T2DM at UP-PGH diabetes clinic and to determine their correlation to physical activity level.
METHODOLOGYSampling and Design of the Study
This is a cross sectional study of adult patients diagnosed with T2DM seen at the PGH diabetes out-patient clinic during the study period of 6 months from September 2015 to February 2016. A total of 151 participants were included (46 males and 105 females). The study subjects were selected on the basis of the inclusion criteria which include age 30 years and above, diagnosed with T2DM and receiving treatment for diabetes, with or without major complications, and willing to participate in the study with the ability to comprehend relevant information. Patients with impaired mental function who were unable to comprehend relevant information, who had life-threatening illnesses, disability, proliferative retinopathy, pregnant women and those who had type 1 diabetes mellitus or other chronic conditions that may influence physical activity such as stroke and cancer were excluded. The study was approved by the PGH Expanded Hospital Research Office (EHRO). Informed consent was obtained from patients before the study began.
Eligible study subjects were interviewed to obtain information on socio-demographic parameters which include age, gender, marital status, educational level, occupational status, and place of residence. HbA1c values were obtained from medical records. Only values recorded for the past three months were used for the study. Measurements of the weight and height were obtained. A face-to-face interview was then made using a validated physical activity questionnaire to assess the physical activity level of the study population.
Study SampleA total of 151 study subjects were included in the study. The minimum sample size requirement was estimated to be at least 96 based on the proportion (45.2%) of physical inactivity in the Philippines among adults (NNS 2013) with a 95% confidence interval, 10% margin of error and 5% level of significance.[12]
Physical Activity MeasurementPhysical activity level of patients with T2DM were assessed using a WHO validated Global Physical Activity Questionnaire (GPAQ). It is composed of 16 questions about physical activity in a typical week and assesses physical activity in three domains, namely, work, transportation and recreational activities. The ratio of a person's working metabolic rate relative to the resting metabolic rate is called metabolic equivalent (MET). In the calculation of a person's overall energy expenditure, 4 METs was given to the time spent in moderate activities, and 8 METs to the time spent in vigorous activities. The total time spent on physical activity during a typical week, the number of days as well as the intensity of physical activity is taken into account to calculate for the categorical indicator. The three levels of physical activity suggested for classifying patients are low, moderate, and high. High if 7 or more days of any combination of walking, moderate or vigorous intensity activities achieving a minimum of at least 3,000 MET-minutes per week; moderate if 5 or more days of any combination of walking, moderate or vigorous intensity activities achieving a minimum of at least 600 MET-minutes per week; and low if a person is not meeting any of the above mentioned criteria.
Anthropometric MeasurementsAnthropometric measurements that were taken include weight and height. Body weight was measured without shoes and with light clothing using a mechanical weighing scale (Detecto, USA). Standing height was measured barefooted with light clothing using a stadiometer. The reading of the weight was recorded to the nearest 0.1 kg whereas the height was recorded to the nearest 0.1 cm. Body mass index (BMI) was calculated using the following formula: weight (kg)/height(m²) and classified accordingly based on Asian criteria: underweight - <18.5 kg/m², normal – 18.5-22.9 kg/m², overweight/pre-obese – 23-29.9 kg/m² and obese - ≥30 kg/m².
Statistical AnalysisThe results were presented as means, percentages and standard deviations. The Chi-square test was used to determine the relationship between socio-demographic information, glycemic control and levels of physical activity. Independent t-test was used to determine the differences in age, BMI and HbA1c in relation to physical activity level.
Ethical ConsiderationAll subjects were informed of the purpose of the study and were asked to sign a standard written consent form prior to data collection. The participation of the eligible subjects was voluntary and without financial compensation. Information was recorded anonymously and confidentiality was assured throughout the study period. This cross-sectional study has been duly reviewed and approved by the Technical Review Board (TRB) and University of the Philippines Manila Research Ethics Board (UPMREB).
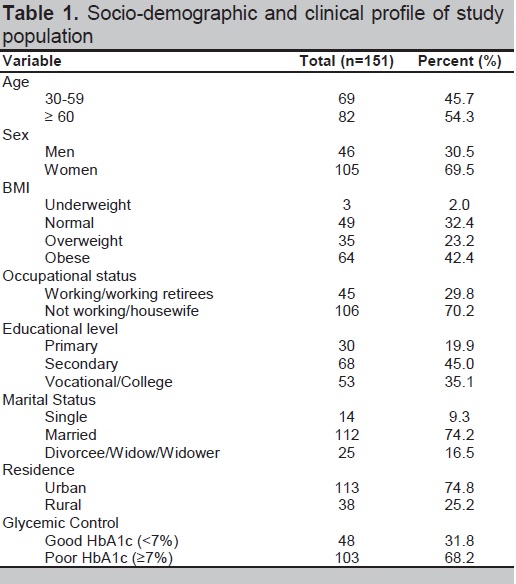
A total of 151 subjects (46 men and 105 women) participated in the study (Table 1). The mean age for the subjects was 59.1 ± 9.5 years and ranged from 31 to 79 years old. Most of the subjects were married (74.2%) and are living in urban areas (74.8%). The majority of the subjects completed secondary education (45%) and were unemployed or housewives (70.2%). About 68.2% of subjects had poor glycemic control based on HbA1c of ≥7%. According to BMI category (Asian criteria), most of the subjects were obese (42.4%).
Click here to download Table 1Table 1.Socio-demographic and clinical profile of study population
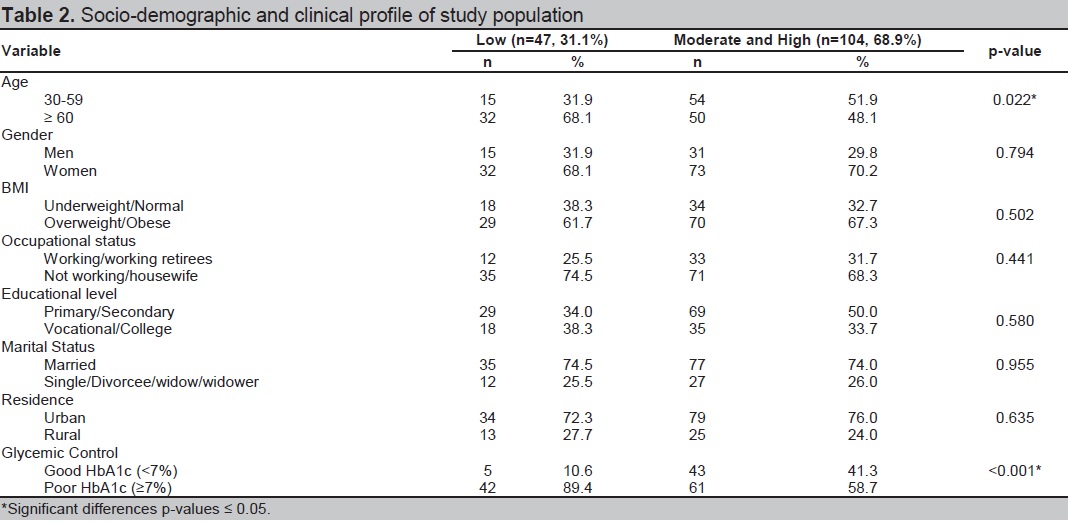
As depicted in Table 2, majority of the patients in UP-PGH Diabetes Clinic had moderate to high physical activity (68.9%). A higher percentage of subjects aged 60 years and above (68.1%; p=0.022) and with poor glycemic control (89.4%; p=<0.001) had low physical activity level as compared to subjects aged 30 to 59 years (31.9%) and with good glycemic control (10.6%) respectively.
Click here to download Table 2Table 2.The proportion of physical activity level relative to clinical profile and socio-demographic profile
Analysis revealed no statistically significant relationship between the level of physical activity, anthropometric profile and other socio-demographic profiles. Table 3 presents the means and standard deviations for age, BMI and glycemic control in relation to physical activity level. The mean age for men and women were 60.9±8.6 years and 57.8±9.9 respectively (p=0.053). Study population with low physical activity had significantly higher HbA1c than those with moderate to high physical activity (7.8±1.6; p=0.001).
Most of the subjects in the study had moderate to high physical activity level (68.9%). Based on the results of the study among adults with diabetes in America, half of the subjects (52.5%) had a moderate physical activity level.[13] A study among adults with T2DM also showed that 64.4% of the patients had moderate physical activity and were not participating in regular exercise.[14] These support the fact that moderate physical activity level is more common among T2DM patients which could be due to the information dissemination of health care providers about the health benefits of doing regular physical activity. It is necessary that physicians, health care workers or educators know about the socio-cultural habits and expected barriers in giving advice to patients with T2DM to enhance adherence to lifestyle modification by developing a diversified and appropriate health education programmes for these high risk group.
In the present study, poor glycemic control was associated with low physical activity level. A study among diabetic patients showed that moderate and vigorous physical activity provides good glycemic control by reducing the value of HbA1c.[15] Physical activity helps in glycemic control by improving insulin sensitivity thus improving glycemic control. In a meta-analysis of 14 clinical controlled trials of physical activity intervention among middle-aged diabetic individuals lasting for about 8 weeks or more demonstrated that regular exercise resulted to a decrease in HbA1c levels.[16] Findings of the available clinical research in knowing the physiologic relationship between diabetes and physical activity still remains insufficient. Aside from searching for complete data of the applicable physiology, we should also give priority towards identifying the strategies on how to encourage our patients to have a sustained exercise that will offer health improvement.
A significantly higher percentage of those aged 60 years and above (68.1%) had lower physical activity than those with younger age group (31.9%). Older age group prefers to do low intensity physical activity because of their perception that diabetes ‘weakened’ and ‘aged’ the body causing them to have some demotivational effect in involving or maintaining a regular exercise regimen and more intense physical activity.[17] Health education plays an important role with emphasis on the necessity of doing regular exercise in preventing and delaying diabetic complications.
The study did not show any association between anthropometric profile and physical activity which was consistent with other similar studies. This might be due to obese individuals who are being motivated to increase their physical activity in order to have weight loss. No significant correlation was also noted between physical activity and other socio-demographic characteristics of the study population.
The limitation of this study is that physical activity was assessed by using a questionnaire which provides a crude measurement of physical activity and is subjected to recall bias. Participation to physical activity itself might be under-reported or over-reported because most of the patients were not able to recall exactly the type and duration of the activity done. Another limitation was the study population was recruited from one diabetes clinic only, which limits the generalizability of the study findings. The results only showed the association of each of the independent variables with the physical activity levels. It is advisable to include dietary history or caloric expenditure and to incorporate accelerometers or pedometers in future studies. Further study is recommended in a multicenter setting with a larger sample size in order to perform a multivariate logistic regression analysis to determine significant associations with different physical activity levels.
The majority of the patients in UP-PGH Diabetes Clinic have moderate to high physical activity. There is no significant relationship between the level of physical activity, anthropometric measurements and other socio-demographic profiles. Subjects with poor glycemic control and older age had low physical activity. Thus, we should promote regular physical activity among diabetic patients with sedentary lifestyle in order to achieve optimal glycemic control and prevent diabetic complications.
Statement of AuthorshipAll authors have given approval to the final version submitted.
Author DisclosureAll the authors have declared no conflict of interest to the work carried out in this paper.
Funding SourceNone.
[1] Diabetes Atlas Committee. Diabetes Atlas, 2nd ed. Brussels, Belgium: International Diabetes Federation. 2003.