Thyroid nodules are prevalent in the general population. The prevalence rates of thyroid nodules range from 2-35% depending on the study population.[1],[2] In the Philippines, the estimated prevalence of nodular goiter is 8.9%.[3] Thyroid nodules are usually asymptomatic but due to the increased use of ultrasound imaging, detection of incidental thyroid nodules has also increased. Ultrasound allows the identification of a wide spectrum of sizes and characteristics that result in difficulty selecting nodules for fine needle aspiration biopsy (FNAB). Sonographic findings suggestive of malignancy are solid nodules, nodule hypoechogenicity or marked hypoechogenicity, irregular margins, microcalcifications and a shape taller than wide on a transverse view.[4] Fine needle aspiration biopsy is a simple procedure and is the preferred initial diagnostic method for the evaluation of thyroid nodules. The sensitivity and specificity for FNAB in published series range between 65% to 98% and 73% to 100%.[5] Histopathology is the gold standard to evaluate the effectiveness of the fine needle aspiration of thyroid nodules to reliably diagnose thyroid malignancy.[6] Most of the thyroid nodules biopsied are benign and only approximately 3-7% of thyroid FNAB are malignant.[7] With this, it is important to use an ultrasound classification that will help differentiate benign from malignant thyroid nodules to decrease unnecessary biopsy.
Several studies regarding Thyroid Imaging, Reporting and Data System (TIRADS) were done since 2009. This was patterned from the widely used and acceptable breast imaging reporting and data system (BIRADS) which showed a number of significant parameters for the quantitative analysis of ultrasound features.[8]-[10] In BIRADS, it is important to differentiate category 3 which is probably benign, from category 4 which is suspicious for malignancy, because management for category 3 is just follow-up imaging, while management for category 4 is biopsy.[11] In a study by Horvath et al., patients with TIRADS 3 should be followed up while patients with TIRADS 4 and 5 nodules must be biopsied or later operated on since malignancy rate for TIRADS 3 was less than 5% while for TIRADS 4 it was at 5-80%.[8]
TIRADS category ranges from TIRADS 1 to TIRADS 5. TIRADS 1 corresponds to normal thyroid gland, TIRADS 2: benign nodules, TIRADS 3: probably benign nodules, TIRADS 4: with ultrasound features suspicious of malignancy, TIRADS 5: nodules highly suggestive of malignancy. Although studies were made regarding TIRADS, they used complex systems which may be difficult to apply in our institution. A study by Horvath et al., was based on 10 ultrasound patterns.[8] Park et al., on the other hand proposed an equation for predicting the probability of thyroid malignancy on the basis of 12 ultrasound features. It is difficult to assign every thyroid nodule into the equation in clinical setting.[9] In a study by Kwak et al., a simpler TIRADS scoring was used based on the BIRADS category such as category 3 (no suspicious US features), 4a (one suspicious feature), 4b (two suspicious features), 4c (three or four suspicious features).[10] This study showed a good correlation of the risk of malignancy using TIRADS scoring.
Filipinos are reported to have a high incidence of thyroid cancer.[12]-[14] In a local study by Puno-Ramos et al., only microcalcification was associated with thyroid malignancy.[15] In a study by Cañete et al., it showed that firm to hard, microcalcification and irregular margins were significant predictors of thyroid malignancy which was similar to international data.[16] However no data regarding the use of TIRADS in a local setting has been reported. Although foreign studies have been done regarding TIRADS, it is important to validate it against local data to determine its applicability in our setting so as to avoid unnecessary biopsy.
The aim of this study is to determine the accuracy of thyroid imaging reporting and data system in detecting thyroid malignancy in comparison to histopathology report.
General ObjectiveTo determine the accuracy of Thyroid Imaging Reporting and Data System (TIRADS) in detecting thyroid malignancy in patients with thyroid nodules
Specific ObjectivesTo determine the ultrasound characteristics of patients with thyroid nodules associated with thyroid malignancy.
To determine the risk of malignancy in each Thyroid Imaging Reporting and Data System (TIRADS) category.
To determine the sensitivity, specificity, PPV and NPV of TIRADS in detecting malignancy of patients with thyroid nodules with surgical histopathology as gold standard.
METHODOLOGYStudy Design
This was a retrospective, cross sectional study approved by our institutional review board. The requirement to obtain informed consent was waived.
Study SubjectsAll Filipino adults who underwent thyroid ultrasound, fine needle aspiration biopsy and thyroidectomy at The Medical City from January 2014 to December 2015 were included in the study.
Study PopulationA minimum of 167 subjects are required for this study based on a level of significance of 5%, a prevalence of 76.13%, sensitivity of 99.6% (95% CI: 98.9-100). The values for the prevalence of malignant nodules and sensitivity of the TIRADS 4 were based from the study by Horvath et al., Prospective validation of the ultrasound based TIRADS classification: results in surgically resected thyroid nodules.
Description of Study ProcedureCytopathology and histopathology records of all patients from January 2014 to December 2015 with thyroid nodules on ultrasound for which FNAB and surgical management were done at The Medical City were gathered from the Department of Clinical Pathology. Patient confidentiality was maintained hence no patient identifiers were used; instead subjects were assigned a number. Records without available digital thyroid ultrasound images and those with indeterminate or suspicious for malignancy on cytology that did not undergo surgery were excluded from the study. Cytopathologic diagnosis was reported using the Bethesda System of classification.[7]
The ultrasound scans of the thyroid gland performed between 2014 and 2015 that were stored in Siemens Syngo Viewer were reviewed. Two radiologists, a resident with four-year training experience and one consultant with more than ten years of experience, reviewed the thyroid ultrasounds. Both were blinded to both the cytopathology and histopathology reports. The two radiologists reviewed the ultrasound imaging on separate occasions. In the event of discrepancies, the reading of the consultant was followed.
All thyroid nodules were characterized according to composition, echogenicity, margins, calcification and shape. Composition was either solid or mixed. A solid nodule was defined as a purely solid or predominantly solid with a cystic component comprising less than 10% of the total volume. Mixed nodule revealed features of both solid and cystic (anechoic on ultrasound).
Echogenicity was either classified as hyperechogenicity, isoechogenicity, hypoechogenicity or marked hypoechogenicity. Hyperechogenicity was defined as echogenicity of the nodule more than that of the adjacent thyroid parenchyma, while isoechogenicity showed similar echogenicity to the surrounding thyroid parenchyma. Hypoechogenicity was characterized as echogenicity less than that of the adjacent thyroid parenchyma but more than that of the surrounding strap muscle, while marked hypoechogenicity was described as echogenicity that was less than the strap muscle.
The margins were classified as regular, microlobulated or irregular. Regular margin was when the border was smooth, distinct, well defined and with regular outline, while microlobulated margin was defined as the presence of many small lobules on the surface of a nodule and irregular margin was when the border is ill–defined, not smooth and with indistinct interface between the nodule and adjacent thyroid parenchyma.
Calcifications when present, were categorized as either microcalcification or macrocalcification. Microcalcifications were described as tiny, hyperechoic foci less than 1.0 mm in size with no comet-tail artifacts while macrocalcifications were hyperechoic foci larger than 1.0 mm. Shape was categorized as taller than wide when anteroposterior dimension was greater than the transverse dimension, while wider than tall was defined as transverse dimension greater than anteroposterior dimension.
Kwak classification was used in this study and nodules were classified into TIRADS category (1, 2, 3, 4a, 4b, 4c, 5) based on ultrasound features.[10]
Data AnalysisFrequency and percentage, mean and standard deviation were used to summarize the clinical characteristics of patients. A two-way table was constructed to determine accuracy measures (sensitivity, specificity, predictive values, likelihood ratios) of TIRADS compared to histopathology. We used simple logistic regression to determine crude associations of surgical histopathologic malignancy with patients’ demographic and clinical characteristics. The ultrasound features associated with malignancy were determined by multiple regression analysis. Crude and adjusted odds ratios and their corresponding 95% confidence intervals were determined. Null hypotheses were rejected at 0.05 alpha level of significance. STATA v12 software was used.
We had a total of 206 patients who underwent thyroidectomy and FNAB, of which 57 patients were excluded because these patients had no thyroid ultrasound reports. We analyzed a total of 149 patients, of whom 50 (33.56%) were confirmed to be malignant via histopathology (Figure 1).
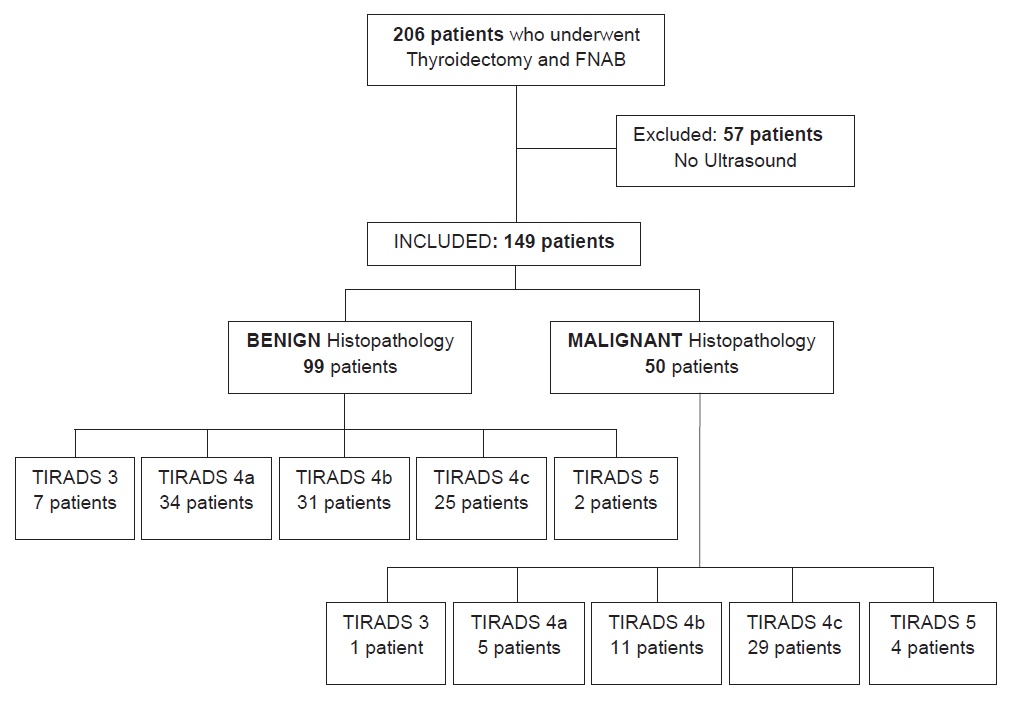
Figure 1. Summary of patient population and TIRADS classification.
Majority of patients were in their 30s (23%), 40s (22%), or 50s (22%). The mean age was 46.91 + 13.57. There were more females (87%) than males. The most frequent characteristics of nodules on ultrasound were solid in composition (62%), hypoechoic (38%) or isoechoic to hyperechoic (36%), well-circumscribed (41%), and wider than tall (83%). Microcalcifications were present in 24% of nodules, while macrocalcifications were seen in 19%. Patients with TIRADS 4a, 4b, and 4c comprised 26%, 28%, and 36% of the group, respectively. About 55% of nodules were classified as benign by Bethesda system after FNAB. On the other hand, final histopathologic diagnosis was benign in 66% of resected specimens (Table 1).
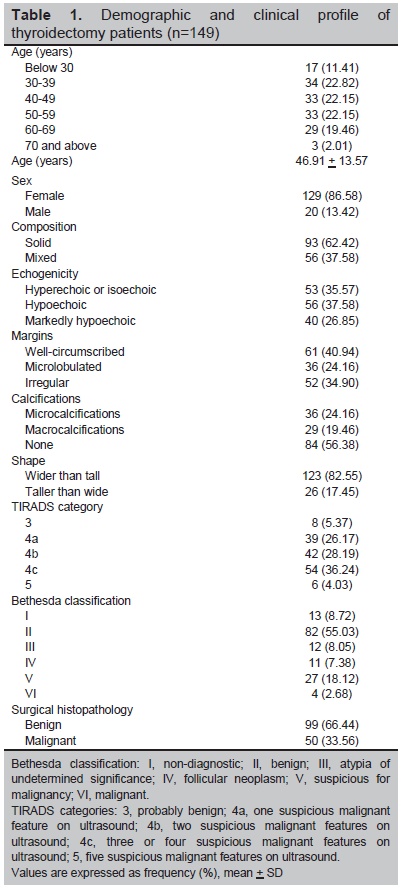
Table 1. Demographic and clinical profile of thyroidectomy patients (n=149)
We compared select characteristics between patients with malignant versus benign thyroid nodules. Compared to mixed nodules, patients with a solid composition was 7.48 times as likely to have a malignant nodule (OR 7.48 95% CI 2.92 to 19.15, p<0.001). Those with markedly hypoechoic nodules were three times more likely to have a malignant nodule (OR 3.42 95% CI 1.40 to 8.25, p=0.007). Nodules with irregular margins were four times more likely to be malignant (OR 3.99, 95% CI 1.76 to 9.05, p=0.001). Compared to patients without calcifications, patients with macrocalcifications were less likely to be malignant (OR 0.34, 95% CI 0.15 to 0.79, p=0.012) (Table 2).
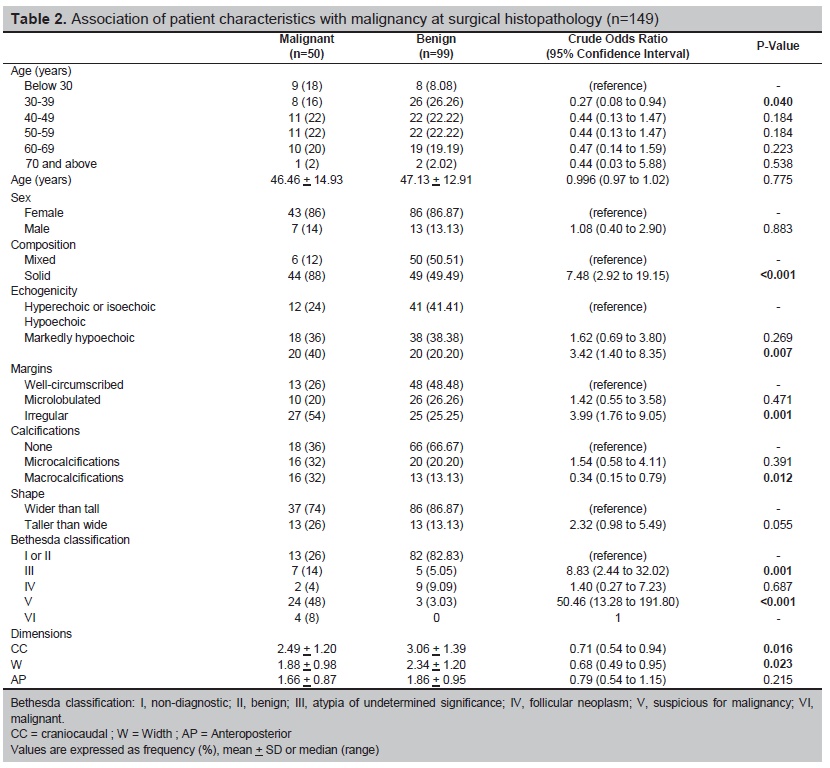
Table 2. Association of patient characteristics with malignancy at surgical histopathology (n=149)
FNAB results according to Bethesda classification were: Bethesda I 8.72%, Bethesda II 55.03%, Bethesda III 8.05%, Bethesda IV 7.38%, Bethesda V 18.12%, Bethesda VI 2.68% (Table 3).
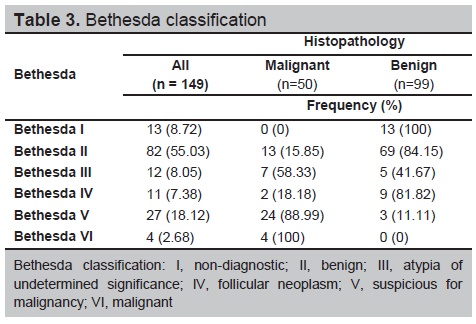
Table 3. Bethesda classification
We conducted a stepwise logistic regression to determine predictors of malignant thyroid nodules. We found the following characteristics to predict malignant nodules: solid composition and higher Besthesda classes (Table 4). Our model explains 40% in the variability of the histopathology results (p<0.001).
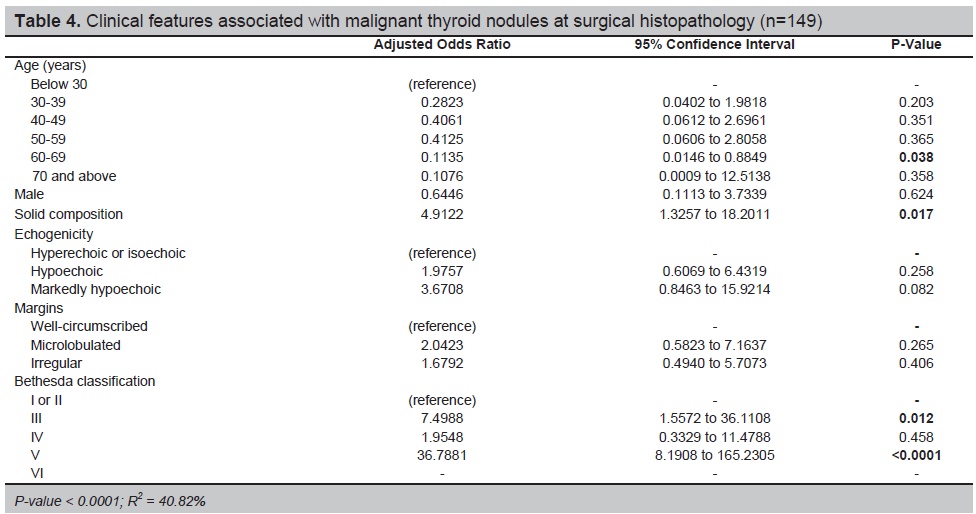
Table 4. Clinical features associated with malignant thyroid nodules at surgical histopathology (n=149)
The malignancy risk of TIRADS category 3, 4a, 4b, 4c and 5 were 12.5% (1 out of 8), 12.82% (5 out of 39), 38.10% (11 out of 42), 57.41% (29 out of 54) and 66.67% (4 out of 6), respectively. The crude odds ratio for TIRADS 4a, 4b, 4c and 5 were: 1.03 (0.10 to 10.23), 2.48 (0.27 to 22.54), 8.12 (0.93 to 70.59) and 14.0 (0.94 to 207.60), respectively. We had insufficient evidence to demonstrate a difference in TIRADS grading distribution between malignant and benign nodules (Table 5).
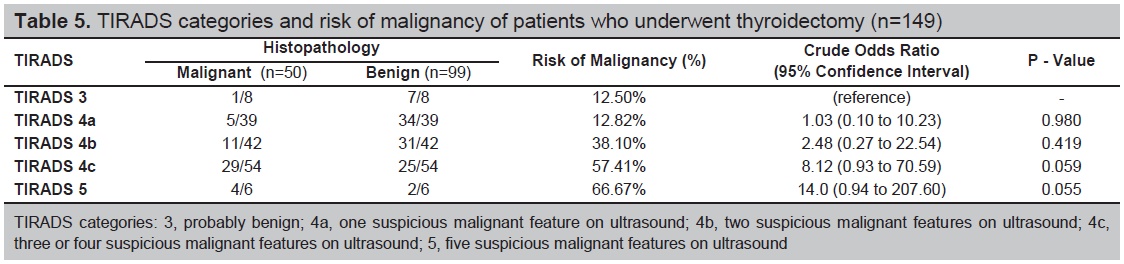
Table 5. TIRADS categories and risk of malignancy of patients who underwent thyroidectomy (n=149)
On comparing TIRADS results and histopathology, we found that TIRADS 4a to 5 classes had approximately 98% sensitivity, 7.07% specificity, LR+ of 1.05, LR- of 0.28, PPV of 34.75%, NPV of 87.5%, and accuracy of 53% (Table 6).
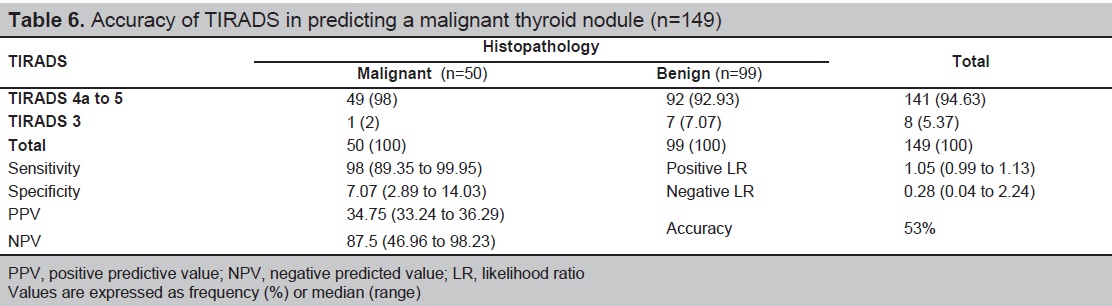
Table 6. Accuracy of TIRADS in predicting a malignant thyroid nodule (n=149)
Ultrasonography of the thyroid gland even in asymptomatic patients increased the detection of thyroid nodules in the general population.[17] Current guideline for adult patients with thyroid nodules and differentiated thyroid cancer by the American Thyroid Association (ATA) 2015 recommended fine needle aspiration biopsy (FNAB) for the following: (1) thyroid nodules measuring 1 cm and above with intermediate to high sonographic pattern; (2) thyroid nodules with low suspicious pattern measuring 1.5 cm and above; and (3) thyroid nodules with very low suspicious ultrasound pattern measuring 2 cm and above.4 Ultrasound features are important in predicting risk of malignancy. According to ATA, high suspicion ultrasonographic pattern is characterized as solid hypoechoic nodule or solid hypoechoic component of a partially cystic nodule with one or more of the following features: irregular margins, microcalcifications, taller than wide shape, rim calcifications with small extrusive soft tissue component and with evidence of extrathyroidal extension.
Intermediate suspicious sonographic pattern is described as thyroid nodules with hypoechoic features with smooth margins without microcalcification, extrathyroidal extension or taller than wide shape.
Low suspicion sonographic pattern is described as isoechoic or hyperechoic solid nodule or partially cystic nodule with eccentric solid areas without microcalcification, irregular margin or extrathyroidal extension or taller than wide shape, while very low suspicion sonographic pattern is characterized as spongiform or partially cystic nodules without any of the sonographic features described in low, intermediate or high suspicion patterns.
The malignancy risks recommended by the ATA are more than 70-90% for the high suspicion pattern, 10-20% for the intermediate suspicion pattern, 5-10% for the low suspicion pattern, less than 3% for the very low suspicion pattern and less than 1% for the benign patern.[4]
In our study, solid composition was 7.48 times likely to have a malignant nodule (OR 7.48 95% Cl 2.92 to 19.15, p <0.001). While those nodules with marked hypoechogenicity were three times more likely to have a malignant nodule (OR 3.42 95% Cl 1.40 to 8.25, p=0.007). Nodules with irregular margins on the other hand were four times more likely to be malignant (OR 3.99, 95% Cl 1.76 to 9.05, p=0.001). But on adjusted OR, solid nodule was the only ultrasound feature predictive of malignancy with OR 4.912 (95% Cl 1.3257 to 18.2011, p=0.017). While a local study published by Puno-Ramos et al., it showed that only the presence of microcalcification on ultrasound had a significant correlation with malignancy with odds ratio of 11.3 and it also showed that a nodule with more than two ultrasound features predictive of malignancy was more likely to be malignant on cytopathology with p-value of 0.00.[15] Smith-Bindman et al., also studied ultrasound imaging characteristics associated with malignant nodules and showed that three ultrasound nodule characteristics which were microcalcification (odd ratio (OR), 8.1; 95% CI, 3.8-17.3), size greater than 2 cm (OR 3.6; 95% CI, 1.7-7.6) and an entirely solid composition (OR, 4.0; 95% CI, 1.7-9.2) were statistically significant in predicting thyroid malignancy.[18] In a meta-analysis done by Remonti et al., on the other hand revealed that solid nodule, hypoechogenicity, irregular margins, absence of halo, microcalcifications, central vascularization, solitary nodule, heterogeneity, taller than wide shape and elasticity were all significantly associated with malignancy with odds ratio (OR) ranging from 1.77 to 35.7. But the sensitivity of ultrasound features predictive of malignancy only ranged from 26.7 to 63% and the author concluded that ultrasound features in isolation do not provide reliable guide as when to do FNAB.[19]
Fine needle aspiration biopsy is the preferred initial diagnostic method for the evaluation of thyroid nodules. Most of the thyroid nodules biopsied are benign and only approximately 3-7% of thyroid FNAB are malignant.[7] The sensitivity and specificity for FNAB in published series range between 65% to 98% and 73 to 100%, respectively.[5] In our study the sensitivity of fine needle aspiration biopsy was 60.00% which was slightly lower than the published series but the specificity was comparable at 87.88% with the published studies. Bethesda Classification I is not an uncommon finding. According to Cibas et al., the risk of malignancy for Bethesda I is at 1-4%.[7] But in the study by Bongiovanni et al., the malignancy rate of nondiagnostic FNAB who underwent surgical excision is approximately 17%.[20] In our study, 8.72% of the patients were classified under Bethesda I, of which all their histopathology reports were not malignant. Our patients classified under Bethesda III on the other hand were eight times likely to have malignant nodules (OR 8.0906 95% Cl 1.6951 to 38.6160, p=0.009) With this, it is important to use an ultrasound classification that will help differentiate benign from malignant thyroid nodules in order to decrease unnecessary biopsy.
Horvath et al., in 2009 first published a study with regards to the use of TIRADS classification. Its main objective was to improve the ultrasound characterization of nodules and establish risk groups for patients who will undergo FNAB.[8] They described 10 ultrasound patterns of thyroid nodules with related risk of malignancy.[8] This was followed by a study by Park et al., which proposed an equation for predicting the probability of malignancy on the basis of 12 ultrasound features.[9] Both studies correlated well with risk of malignancy, however these ultrasound patterns and equations were cumbersome and complex and are not applicable to all thyroid nodules nor in clinical practice. Hence Kwak et al., investigated a practical TIRADS classification for the management of thyroid nodules. Sonographic characteristics predictive of malignancy such as: solid echogenicity, hypoechogenicity or marked hypoechogenicity, microcalcifications, microlobulated or irregular border and taller than wide shape were used to classify TIRADS from 1 to 5. They categorized the TIRADS to 1: normal thyroid gland, 2: benign nodules, 3: probably benign nodules, 4a: one ultrasound feature suggestive of malignancy, 4b: two ultrasound features suggestive of malignancy, 4c: three or four features suggestive of malignancy and 5: five ultrasound features suggestive of malignancy.[10] The study of Kwak et al., revealed that TIRADS 3 or nodules with no ultrasound features suggestive of malignancy had a fitted probability of malignancy of 0.02-0.028 indicating that biopsy may not be necessary while for nodules with TIRADS 4-5, it had a fitted probability of malignancy of 0.036 for which FNAB is indicated and the results were comparable with the widely accepted BIRADS.[10] In a prospective study by Srinivas et al., they used the TIRADS classification as suggested by Kwak et al., and showed that the classification is a reliable modality in differentiating benign nodules from malignant nodules.[21]
Our study adapted the TIRADS classification used by Kwak et al. It showed that the malignancy risk of TIRADS category 3, 4a, 4b, 4c and 5 were 12.5% (1 out of 8), 12.82% (5 out of 39), 26.19% (11 out of 42), 53.70% (29 out of 54) and 66.67% (4 out of 6), respectively. Since majority of the population had at least one ultrasound feature suggestive of malignancy and only 8 patients had TIRADS 3, the malignancy risk of TIRADS 3 was higher compared to other studies.[8]-[10],[21]-[24] The histopathology report of the patient who had a malignant result showed follicular carcinoma on top of a micropapillary carcinoma. One patient who also had TIRADS 3 had an incidental finding of micropapillary carcinoma measuring 0.5 cm within the left lobe but the FNAB was done on another nodule that measured 1.87 cm x 1.53 cm x 1.06 cm (CC x W x AP) in the right lobe. The crude odds ratio for TIRADS 4a, 4b, 4c and 5 were: 1.03 (0.10 to 10.23), 2.48 (0.27 to 22.54), 8.12 (0.93 to 70.59) and 14.0 (0.94 to 207.60), respectively. We had insufficient evidence to demonstrate a difference in TIRADS grading distribution between malignant and benign nodules.
The accuracy of TIRADS in our study was 53% which was slightly lower as compared to the studies of Ha et al., at 69.5%[22] and Russ et al., at 62%.[25] The reason for low accuracy is possibly because of a high false positive rate. The overall sensitivity of TIRADS categories 4 and 5 for malignancy was 98.00% which was higher than that reported by Ha et al., (95.5%)[22] and Yoon et al., (97.4%).[24] Although the PPV of this study was 34.75% which was lower as compared to PPVs of Horvath et al.,[8] and Ha et al.,[22] (49% and 44.5% respectively). The specificity of this study was only 7.07% which was also lower compared to other studies (29%-75%).a href="#_edn8" name="_ednref8" title="">[8],[22]-[24]
In our study, the prevalence of malignancy was higher at 33.56% compared to an FNAB based series wherein malignancy rate was only 3 to 7%.[7] With this, PPV/NPV might be affected since an increase in prevalence leads to increase in PPV. The implication is that a screening test is more efficient in a high risk target population. If the prevalence of the disease is low, the positive predictive value will not be high even if both the sensitivity and specificity are high. When screening the general population, many people with positive test results will be false positives.[26]
Despite the relatively low accuracy, this study showed that TIRADS is a useful screening tool to defer the need for fine needle aspiration biopsy for patients with TIRADS 3 classification. The number of ultrasound features predictive of malignancy is an important guide in determining further management as to whether to observe the nodules or do appropriate intervention such as fine needle aspiration biopsy.
This study showed that presence of solid nodule in the thyroid is predictive of thyroid malignancy. Higher TIRADS classification is associated with higher risk of thyroid malignancy. TIRADS is a sensitive classification in recognizing patients with thyroid cancer and can be used as a guide in deciding the need for fine needle aspiration biopsy.
Ultrasound features such as markedly hypoechoic nodules and nodules with irregular borders were associated with increased likelihood of malignancy but did not reach statistical significance in multivariate analysis.
Limitations of the Study and RecommendationsThe investigators identified a number of limitations to this study. First, the results showed a wide confidence interval which was reflective of a relatively small sample size. Second, this was a retrospective study hence there might be selection bias. All our subjects underwent surgery due to the presence of ultrasound features suggestive of malignancy. Hence, it is worth mentioning that our malignancy rate is higher at 33.56% as compared to an FNAB based series wherein malignancy rate is only 3 to 7%.[7] Third, the study did not represent equally the different TIRADS categories since majority of the population had at least 1 suspicious ultrasound feature suggestive of malignancy. Fourth, it is from a single institution which might not be reflective of the entire population. In order to validate our findings, we recommend a prospective multicenter study in evaluating the use of TIRADS. Once validated, TIRADS may be used as a reference for reporting thyroid pathology and implemented as a standardized coding for all clinicians and radiologists.
AcknowledgmentsThe authors thank Pier Angeli D. Medina, MD and Elizabeth Ann S. Alcazaren MD for providing the cytopathology and histopathology records of patients in this study.
Statement of AuthorshipAll authors certified fulfillment of ICMJE authorship criteria.
Author DisclosureThe authors declared no conflict of interest.
Funding SourceNone.
[1] Ezzat S, Sarti DA, Cain DR, Braunstein GD. Thyroid incidentalomas. Prevalence by palpation and ultrasonography. Arch Intern Med. 1994; 154(16):1838-40. PubMed.