The prevalence of diabetes mellitus (DM) is increasing rapidly all over the world. Asian countries account for more than 60% of the world’s diabetic population.[1] The prevalence estimate published by the International Diabetes Federation reported that there were 3.5 million cases of DM in the Philippines in 2015 with a prevalence of 6.1% in adults.[2] A study conducted in six national regions of the Philippines showed that the 9-year incidence and prevalence of type 2 diabetes mellitus (T2DM) wereas quite high (16.3% and 28.0%, respectively).[3] Currently, there is no nationwide published data on the prevalence and incidence of type 1 diabetes mellitus (T1DM) in the Philippines.[4] International Diabetes Federation data on diabetes in young patients projected an increase in the incidence of T1DM in the coming years, with Southeast Asian countries expected to contribute the largest (24%) to the young diabetic population.[5],[6]
Insulin therapy is the most common treatment option for patients with T1DM, and also in patients with T2DM, especially in cases where oral anti-diabetes therapies fail.[7] Hypoglycemia is an important complication of insulin therapy. The fear of hypoglycemia often prevents or delays the decision of patients and healthcare providers to prescribe insulin, thus adding to the burden of poor DM control.[8] Philippine practice guidelines for diabetes management also encourage patients to self-monitor blood glucose (SMBG) when they are on insulin therapy or have risks of hypoglycemia.[7] Hypoglycemia tends to increase with increased duration of insulin usage in patients, as was reported in the UK Hypoglycemia Study Group. A high prevalence of severe hypoglycemia (25%) was seen in patients with T2DM who were on insulin for more than 5 years.[9] Hypoglycemia impacts daily activity and productivity in patients with T1DM and T2DM. It also increases fear and anxiety in patients with DM and consequently healthcare costs.[10]
The seemingly high prevalence of DM in the Philippines and the impact of hypoglycemia on the socio-economic growth of the country necessitate detailed evaluation of hypoglycemia in the Philippine population so that steps can be taken for better management of hypoglycemia. However, no such studies (observational or clinical) has been conducted so far in the Philippines which will provide an estimate regarding incidence of hypoglycemia or its impact on daily activities and healthcare utilization. This is the first study that provides patient-reported hypoglycemic rates in Filipino patients with DM using a questionnaire data set.
The Global Hypoglycemia Assessment Tool (HAT) study collected data from insulin-treated patients with DM in 24 countries, and showed that rates of hypoglycemia were higher than had been reported previously.[11] The non-interventional International Operations HAT (IO HAT) study assessed incidence of hypoglycemia in insulin-treated patients with DM in Bangladesh, Colombia, Egypt, Indonesia, Philippines, Singapore, South Africa, Turkey and the United Arab Emirates.[12] The IO HAT study was built on the information gathered from the Global HAT study. Here we report the results of the Philippine cohort of IO HAT.
METHODOLOGYStudy design
The IO HAT study design is described in Figure 1. This is a cohort study that involved both a retrospective cross-sectional and prospective observational evaluation. In this cohort, hypoglycemia data were collected from patients recruited at 39 sites in the Philippines from 21 endocrinologists and 18 diabetes specialists between 01 Jan 2015 and 14 May 2015. This study was conducted in accordance with Good Pharmacoepidemiology Practices, Declaration of Helsinki, and Ethical Principles for Medical Research Involving Human Patients.[13],[14]
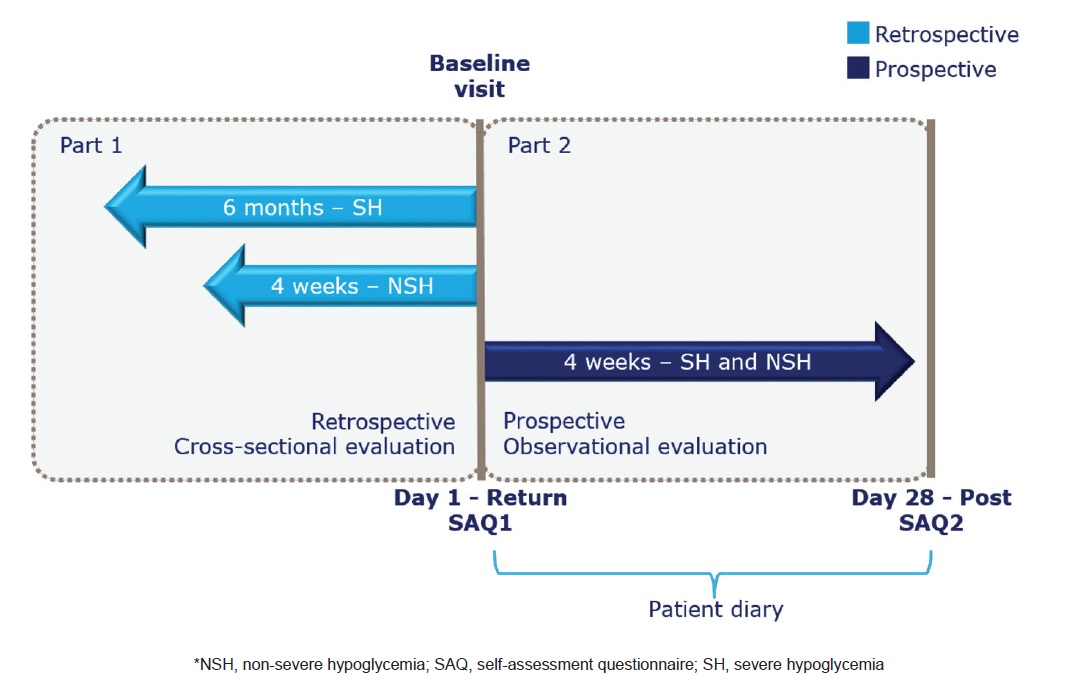
Figure 1. IO HAT study design. This study involved both retrospective cross-sectional and prospective observational evaluation, assessed using two-part self-assessment questionnaires (SAQ1 and SAQ2) and patient diary’s that recorded hypoglycemia during retrospective (6 months/4 weeks before baseline) and prospective period (4 weeks after baseline).[12]
Patients
Ambulatory and literate Filipino male or female patients with T1DM and T2DM, aged 18 years or older, treated with insulin for more than 12 months, and who had signed informed consent were included in this study. Participating patients were enrolled consecutively as a result of attendance to a routine clinic appointment. Participation in the study was dependent on having a sufficient duration of insulin use, but was not dependent on the use of any specific medicinal product. The investigators were primarily endocrinologists and diabetologists; however, a few internal medicine physicians (internists) also participated.
Study assessments
Endpoints:
This study comprised of a two-part self-assessment questionnaire (SAQ) including a retrospective cross-sectional evaluation (SAQ1) and a prospective observational evaluation (SAQ2). SAQ1 (includes 34 questions) assessed baseline demographic and treatment information, hypoglycemia unawareness and perceptions of hypoglycemia, history of severe hypoglycemia for 6 months before the baseline visit, and “any” and “nocturnal” hypoglycemia for 4 weeks before the baseline visit. SAQ2 (includes 6 questions) assessed severe and symptomatic hypoglycemia and its effect on productivity and healthcare utilization for 4 weeks from the baseline visit. Patients answered these questions using a 6-point Likert scale, with responses corresponding to agreement with each item statement ranging from ‘‘very strongly agree” (score = 5) to ‘‘do not agree at all” (score = 0). The validated questionnaires were translated into Filipino language with reference to WHO approved international guidelines for translation and cultural adaptation of questionnaires.
The primary endpoint of the study was the percentage of patients who experienced at least one hypoglycemic episode during the 4-week prospective period. Secondary endpoints included, difference in incidence rates of any, nocturnal, and severe hypoglycemia between two periods of observation (i.e., retrospective and prospective); relationship between diabetes treatment; glycated hemoglobin (HbA1c) at baseline (HbA1c <7.0%, 7.0% to 9.0%, and >9.0%); and hypoglycemic events. The patients’ knowledge of hypoglycemia, hypoglycemia unawareness, fear of hypoglycemia, patients’ action resulting from hypoglycemia, and its impact on work/study and health system resources were also assessed.
Hypoglycemia awareness was assessed and categorized in to the following: ‘normal’, ‘impaired’, and ‘severely impaired’ based on patients’ responses to the question. Fear of hypoglycemia was assessed on visual analogue scale (0 to 10), where ‘0’ denotes ‘not afraid at all’ and ‘10’ denotes ‘absolutely terrified’.
Hypoglycemia definition
The following definitions of hypoglycemia were employed in this study to capture the different types of hypoglycemia in SAQ and patient diary (PD):
Severe hypoglycemia: An event requiring the assistance of another person to actively administer carbohydrate, glucagon, or take other corrective actions (as per ADA definition of severe hypoglycemia).[15] Nocturnal hypoglycemia: A hypoglycemic event occurring between midnight and 06:00 hours. Any hypoglycemia: Aggregate of all hypoglycemic events of any category, calculated based on questionnaire and PD entries.
Statistical analysis
All statistical tests were two-sided, with the criterion for statistical significance set at p <0.05. No adjustment were made for multiple comparisons. For the primary endpoint, the percentage of patients who experienced at least one hypoglycemic episode during the 4-week prospective observational period was calculated together with 95% confidence interval (CI) for this percentage. For secondary endpoints, the incidence of various types of hypoglycemia was calculated as number of episodes per patient year (events PPY) (together with the 95% CI), expressed by the formula: Incidence rate (IR) = total number of events divided by total follow-up time (patient-years). Incidence rate ratio, 95% CI for incidence rate ratio, and p-value for incidence rate ratio were calculated using a negative binomial regression model including a single binary covariate for period (4 weeks before baseline, 4 weeks after baseline), specifying a log transformed exposure time offset term and using robust standard errors to adjust for repeated measurements on individuals. The scatter plot with regression line and 95% CI was utilized to study the relationship between HbA1c at baseline and log-transformed number of events for patients experiencing hypoglycemia in the retrospective and prospective periods. Given that the majority of analyses were descriptive in nature, no imputation of missing data was performed. Baseline refers to data collected using SAQ1; follow-up refers to data collected using SAQ2 and, where applicable, PD.
Patient characteristics
A total of 671 patients (T1DM: 62; T2DM: 609) were enrolled from study sites in the Philippines and completed SAQ1. A total of 637 patients (T1DM: 57; T2DM: 580) completed SAQ2. Table 1 describes the baseline demographic details of Filipino cohort. The duration of diabetes in T1DM and T2DM patients was 12.3 years and 12.9 years, respectively, whereas, the mean HbA1c levels in both the groups were 8.6% and 8.4%, respectively. The mean BMI was high in T2DM patients (26.8 kg/m2) when compared to T1DM patients (21.9 kg/m2). At baseline, in patients with T1DM and T2DM, the most common insulin treatment was pre-mixed insulin (45.2% and 40.2%, respectively) (Table 1). In this cohort, analogue insulin was used by 76.1% of patients and human insulin was used by 23.9% of patients.
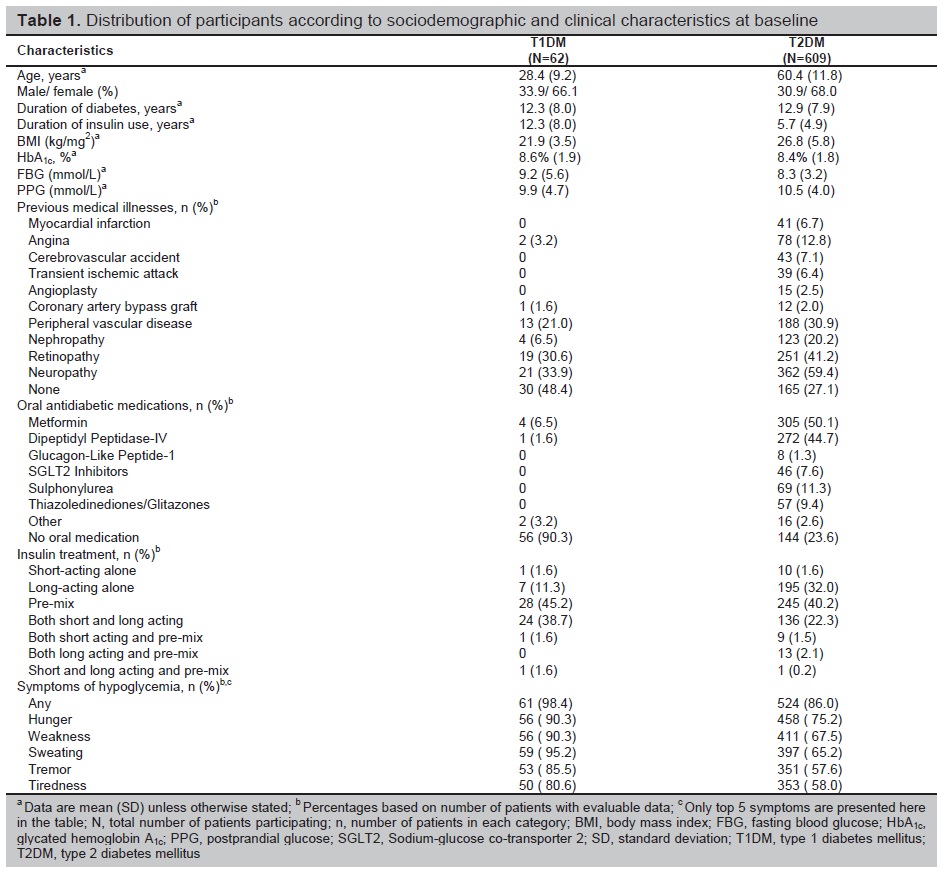
Table 1. Distribution of participants according to sociodemographic and clinical characteristics at baseline
Incidence of hypoglycemia by diabetes type and insulin regimen
It was observed that the rates of ‘any’ and ‘severe’ hypoglycemia were lower in the retrospective period than in the prospective period. However, the rates of nocturnal hypoglycemia were mostly comparable in these two periods.
Any hypoglycemia
In patients with T1DM, all patients (100% [95% CI: 93.7%, 100.0%]) experienced at least 1 hypoglycemic event prospectively (4 weeks after baseline) (Figure 2a). The incidence rate of any hypoglycemia was significantly higher in prospective period as compared to retrospective period (72.6 [95% CI: 64.8, 80.9] events PPY vs. 43.6 [95% CI: 37.8, 49.9] events PPY; p=0.001, respectively). The incidence rate for combination of short- and long-acting insulin regimen was 76.5 events PPY and for pre-mixed regimen was 76.2 events PPY in the prospective period.
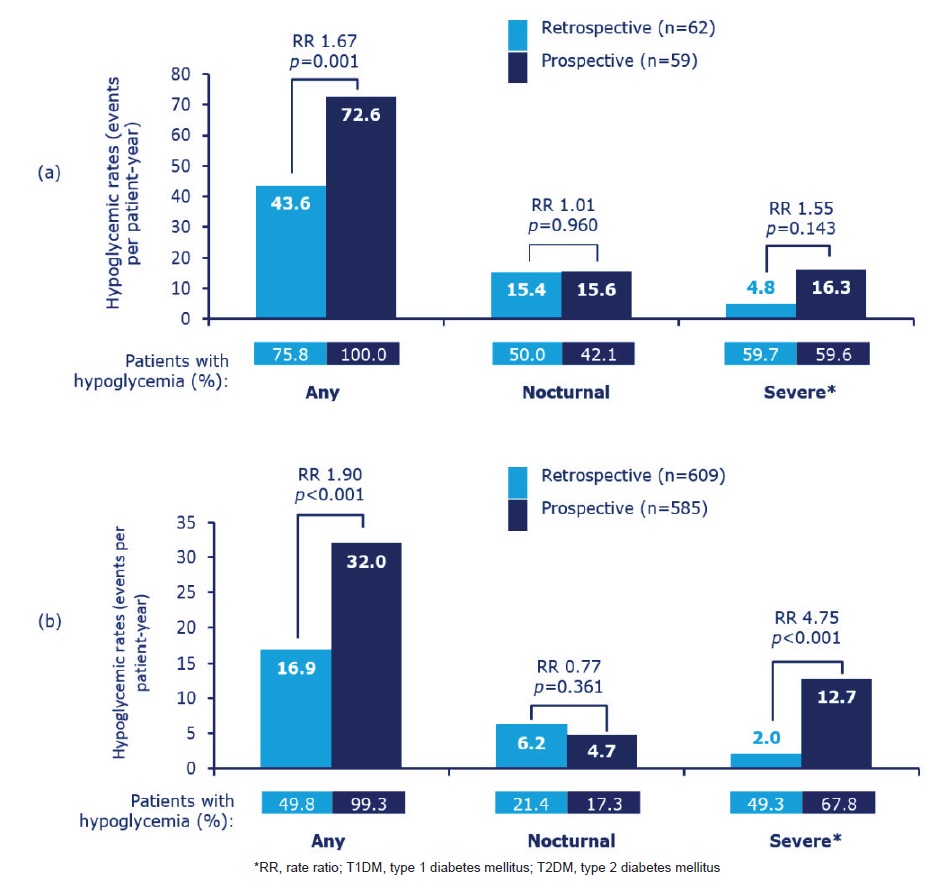
Figure 2. Estimated rate of retrospective and prospective hypoglycemia in (a) patients with T1DM and (b) patients with T2DM. Data based on 4-week period for both retrospective and prospective analyses for any or nocturnal hypoglycemia. Retrospective data based on 6-month period and prospective data based on 4-week period for severe hypoglycemia; RR, rate ratio.
Similarly, patients with T2DM reported significantly higher incidence rates of any hypoglycemia prospectively than retrospectively (32.0 [95% CI: 30.4, 33.7] events PPY vs. 16.9 [95% CI: 15.7, 18.1] events PPY; p<0.001), with almost all (99.3% [95% CI: 98.2%, 99.8%]) patients reporting hypoglycemia in the prospective period (Figure 2b). The incidence rate for pre-mixed insulin regimen was 37.7 events PPY in the prospective period and 21.6 events PPY in the retrospective period (Figure 3a).
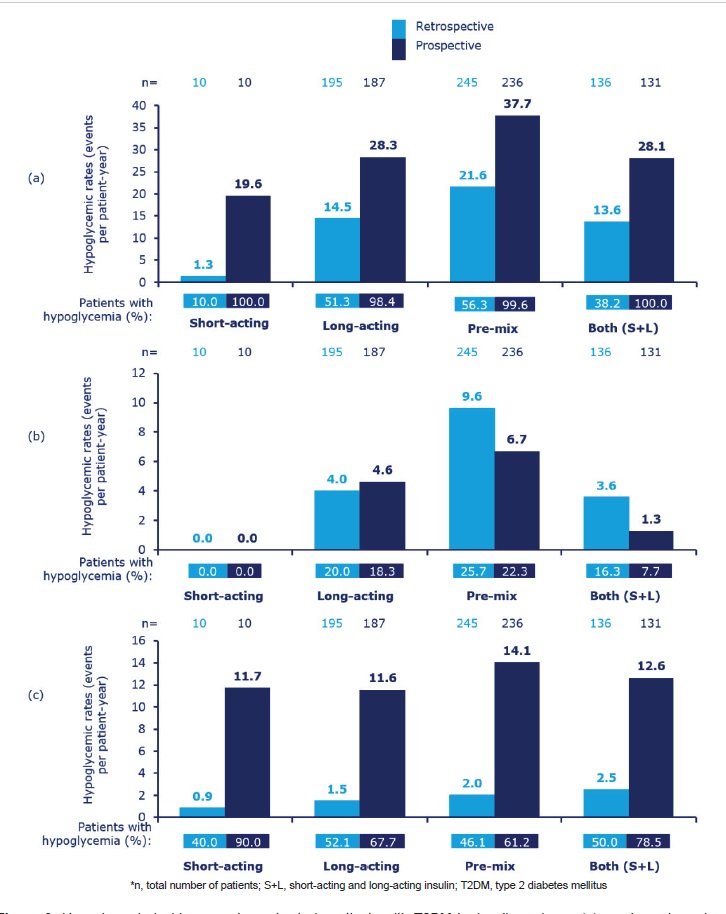
Figure 3. Hypoglycemia incidence and event rate in patients with T2DM by insulin regimen: (a) any hypoglycemia, (b) nocturnal hypoglycemia, (c) severe hypoglycemia. Data based on 4-week period for both retrospective and prospective analyses for any or nocturnal hypoglycemia. Retrospective data based on 6-month period and prospective data based on 4-week period for severe hypoglycemia.
Nocturnal hypoglycemia
In patients with T1DM, there was no significant difference in the incidence rates between the retrospective and prospective periods (15.4 [95% CI: 12.0, 19.3] events PPY vs. 15.6 [95% CI: 12.1, 19.7] events PPY, respectively; p=0.960) (Figure 2a). The incidence rate for long-acting insulin was 22.4 events PPY in the prospective period followed by pre-mixed insulin regimen (21.0 events PPY and 19.3 events PPY) in the retrospective and prospective periods, respectively. In T2DM patients, the incidence rates were not significantly differing from retrospective (6.2 [95% CI: 5.5, 6.9] events PPY) and prospective (4.7 [95% CI: 4.1, 5.4] events PPY, p=0.361) periods (Figure 2b). Overall, the incidence rate of nocturnal hypoglycemia was quite low in patients with T2DM for all insulin regimens (Figure 3b).
Severe hypoglycemia
In patients with T1DM, there was no significant difference in the incidence rates of severe hypoglycemia in retrospective (16.3 [95% CI: 12.7, 20.5] events PPY) and prospective (4.8 [95% CI: 4.0, 5.6] events PPY, p=0.143) period (Figure 2a). In contrast to the observations seen for any and nocturnal hypoglycemia, the incidence rate of severe hypoglycemia was 26.1 events PPY for short-acting insulin regimen prospectively.
Patients with T2DM reported significantly higher rates of severe hypoglycemia prospectively than retrospectively (12.7 [95% CI: 11.7, 13.8] events PPY vs. 1.9 [95% CI: 1.8, 2.1] events PPY, respectively; p<0.001) (Figure 2b). The T2DM patients with all insulin regimens reported incidence rates of 0.9 events PPY to 2.5 events PPY and 11.6 events PPY to 14.1 events PPY with severe hypoglycemia in the retrospective and prospective periods, respectively (Figure 3c).
Relationship between HbA1c at baseline and hypoglycemia rates
No notable relationship was observed between baseline HbA1c (whether treated categorically or as continuous data) and the percentages of patients with hypoglycemia, in T1DM (r2 = 0.0198) and T2DM (r2 = 0.0023).
Patients’ perspectives on hypoglycemia
Patients’ perspectives, including patient knowledge, hypoglycemia awareness, fear of hypoglycemia, response to hypoglycemia, and impact of hypoglycemia on the medical system, are described in Table 2 and Table 3.
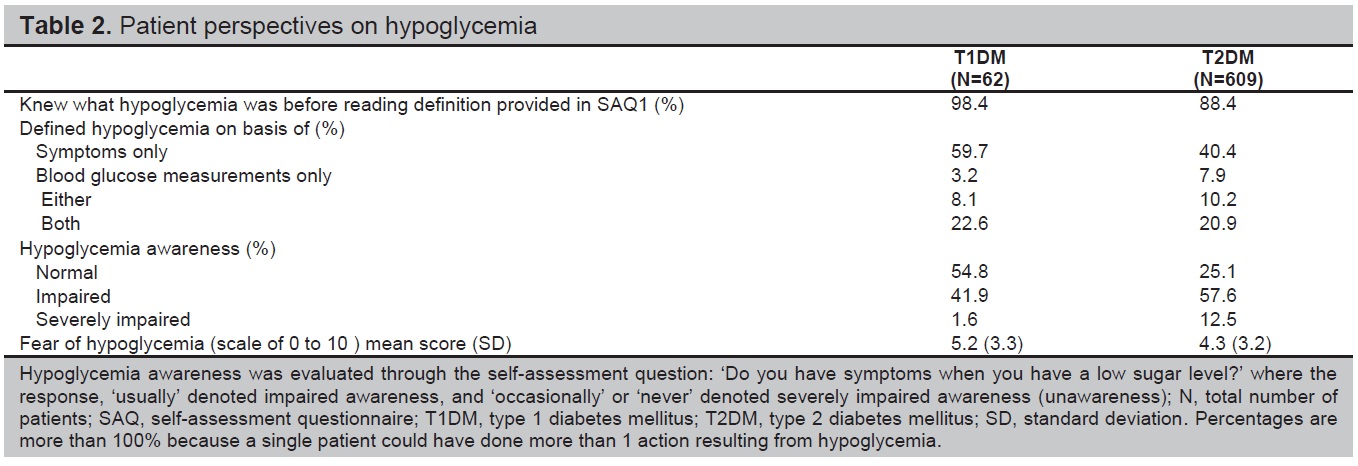
Table 2. Patient perspectives on hypoglycemia
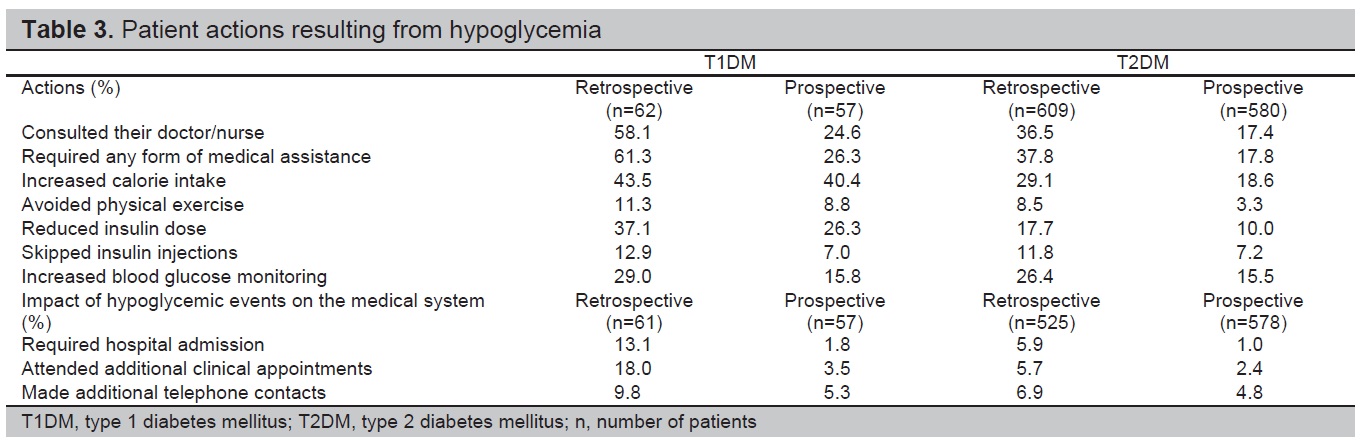
Table 3. Patient actions resulting from hypoglycemia
Impact of hypoglycemic events on work and study
Prior to baseline, 40 out of 62 patients with T1DM and 171 out of 609 patients with T2DM were studying or in full- or part-time employment. A greater percentage of patients with T1DM compared to T2DM experienced hypoglycemic events that resulted in absence from work or studies (22.5% vs. 8.2%, respectively), late arrival to work or study (32.5% vs. 8.2%, respectively), or early departure from work or study (15.0% vs. 11.1%, respectively) in the retrospective period. Figure 4, represents the impact of hypoglycemic events on work and studies in retrospective and prospective period.
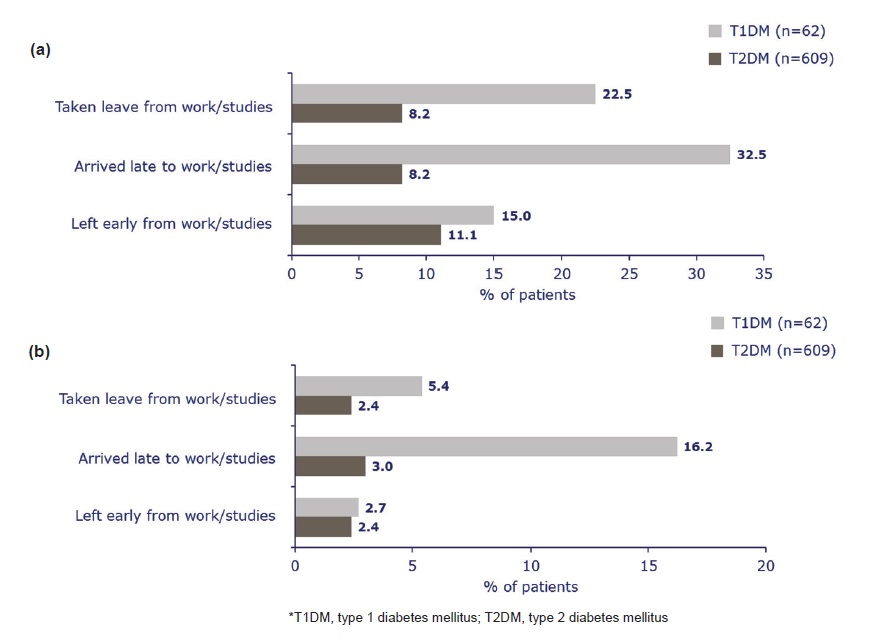
Figure 4. Impact of hypoglycemic events on work and study in (a) retrospective and (b) prospective periods. ‘n’ values represent the number of patients studying or in full or part-time employment and completed Part 1 SAQ. Bars represent proportion of subjects responding ‘Yes’.
This study is a sub-analysis of the Philippine cohort of a multicenter, international, 6-month retrospective and 4-week prospective study with a two-part SAQ that investigated the incidence of hypoglycemia and its impact on daily activities and healthcare resources in insulin-treated adults with T1DM or T2DM. Consistent with the overall IO HAT study results, higher incidence rate of hypoglycemia was reported prospectively when compared with retrospectively, with almost all patients reporting at least one hypoglycemic event during the prospective period (T1DM: 100%; T2DM: 99.3%).[12] This could be due to the use of PD’s in prospective period which assisted recall. In contrast, the retrospective data were only collected by SAQs and were, therefore, prone to recall bias. Contrary to the overall hypoglycemic data, the proportion of patients reporting nocturnal hypoglycemia was statistically equal in both retrospective and prospective periods.
The incidence rate of severe hypoglycemia was also higher during the prospective period than during the retrospective period in patients with T2DM. The recall bias for the retrospective period could be more pronounced for severe hypoglycemia since the period of recall was greater than that of any hypoglycemia (6 months vs. 4 weeks, respectively). Overall, high incidence of any or severe hypoglycemia in the prospective period could be due to combined use of PD and SAQs in this period, which act as a means for patient education, increase in knowledge and awareness of hypoglycemia. This point highlights the significance of patient education, as increased awareness will ensure better reporting of hypoglycemia and, in turn, management of DM by the healthcare providers.
The results also indicate that hypoglycemia is often under-reported by patients retrospectively, and therefore, may have been underestimated in previous studies.
Overall, the incidence of any hypoglycemia in this cohort was quite high in both the groups from retrospective period to prospective period, similar to observations seen in Global HAT study.[11] In an observation study conducted by Donnelly et al., patients with T1DM and T2DM also reported high incidence rates of overall hypoglycemia (42.89 events PPY and 16.37 events PPY, respectively); however, incidence rates of severe hypoglycemia were low (1.15 events PPY and 0.35 events PPY, respectively).[16] Data from the European cohort of PREDICTIVE study reported that overall hypoglycemic events 4 weeks before baseline were 47.5 events PPY for patients with T1DM and 9.2 events PPY for patients with T2DM.[17] The incidence rates of severe hypoglycemia in ACCORD, ADVANCE, and VADT trials with intensive treatment were quite low in comparison to what was observed in our study (0.6 to 12.0 events 100 patients/year).[18],[19],[20] As observed with Global HAT study and Canadian HAT program, the incidence rates of hypoglycemia were higher in patients with T1DM in comparison to T2DM in this cohort.[11],[21] High incidence of severe hypoglycemia in patients with T2DM could be due to patient understanding of ADA definition of severe hypoglycemia, which means that patients could have misunderstood the events as severe only on the basis of assistance received rather than based on severity of symptoms.
Similar to the results from DiabCare study, majority of patients in this study were on pre-mixed insulin at baseline (T1DM: 45.2%; T2DM: 40.2%).[22] However, no statistical testing was done for insulin regimens and also for T1DM vs T2DM patients. The higher incidence rates of any hypoglycemia were reported with pre-mixed insulin in this study. This highlights the need for creating physician awareness in the region and need to shift to insulins with lower associated rates of hypoglycemia such as those based on modern insulin analogues or using insulin-pumps in conjunction with continuous glucose monitoring devices in patients with T1DM.[23],[24],[25] The results from the A1cheive sub-analysis showed that use of basal insulin analogue such as insulin detemir was associated with better glycemic control and lower incidence of hypoglycemia in patients with T2DM in the Philippines.[26]
Based on previous evidence like that from DCCT trial, it is believed that the risk of hypoglycemia was inversely associated with HbA1c levels.[27] However, similar to the results from overall IO HAT study, the results from this cohort also did not report any significant relationship between HbA1c levels at baseline and hypoglycemia rates. Hence, it is important for the healthcare provider to proactively screen patients for hypoglycemia regardless of their HbA1c values.
Hypoglycemic events remarkably impact daily activities and productivity, and add to healthcare burden with increased utilization of resources.11-13 Results from this study showed that the impact on productivity and medical system was greater in patients in the retrospective period compared to the prospective period, suggesting that increased awareness in prospective period may have played a role in improving the quality of life of the patients.
The results also showed that patient knowledge of hypoglycemia was high at baseline in both groups, but majority of patients with T2DM had impaired hypoglycemia awareness (57.6%). As expected, the majority of patients with impaired hypoglycemia awareness are less likely to report incidence of hypoglycemia. Another important observation was that almost all the patients in both the groups who were using blood glucose measurements to report hypoglycemia provided values consistent with standard definition. This reiterates the fact that SMBG should be encouraged in insulin-treated patients and in those at high risk of hypoglycemia.
Recall bias observed during retrospective period is one of the limitations of the study, preventing direct comparison of the data in the prospective and retrospective periods. Patient diaries used in the prospective period assist in patient recall and may also lead to over estimation of hypoglycemia rates. The findings from this study highlight that increased patient knowledge of hypoglycemia, proper tailoring of insulin or choice of insulin, and access to home glucose-monitoring equipment are important considerations that may help reduce the incidence of hypoglycemia.
Consistent with the overall IO HAT study results, higher rates of hypoglycemia were reported prospectively as compared to retrospectively. Hypoglycemic events remarkably affected daily activities, productivity, and medical system utilization and that the high incidence of hypoglycemia seen prospectively may be due to patient education. Results from this study can be used as a tool to educate patients and physicians regarding the importance of hypoglycemia recognition and management.
AcknowledgmentsStatistical analysis was performed by Paraxel International. The authors acknowledge medical writing and submission support provided by Maruthi Prasanna from Cognizant Technology Solutions, funded by Novo Nordisk.
Statement of AuthorshipAll authors certified fulfillment of ICMJE authorship criteria.
Author DisclosureNovo Nordisk was involved in the study design; collection, analysis and interpretation of data; and decision to submit the article for publication.
Authors, Drs. Anand Jain and Arvind Vilas Gadekar are employees of Novo Nordisk. Dr. Roberto Mirasol is a member of the advisory board of Novo Nordisk, Eli Lilly, Astra Zeneca, and Merck. Dr. Nemencio Nicodemus, Jr. is a member of the local advisory board of the following companies: Novo Nordisk, Astra Zeneca, Merck, Torrent and has received speaker honoraria from Novo Nordisk, Astra Zeneca, Merck, Torrent, Eli Lilly, Sanofi, LRI-Therapharma, and Servier. Dr. Susan Yu-Gan has received speakers fee from Novo Nordisk and she has taken part in advisory boards for Novo Nordisk Philippines.
Funding SourceNovo Nordisk provided financial support for the conduct of the research.
[1] Ramachandran A, Chamukuttan S, Shetty AS, Nanditha A. Trends in prevalence of diabetes in Asian countries. World J Diabetes. 2012;3(6):110-7. PubMed Central CrossRef