Although hypercalcemia caused by primary hyperparathyroidism (PHPT) is common, advanced hyperparathyroid skeletal manifestations are now rarely encountered, due to the higher rate of early diagnoses and successful definitive surgical treatments.[1] Unfortunately, PHPT secondary to elusive parathyroid adenomas has remained a challenging entity, presenting a dilemma to endocrinologists managing these patients.[2] Here, we present a rare complex case of PHPT with elusive parathyroid adenomas complicated by florid advanced skull manifestations causing communicating hydrocephalus.
CASEA 47-year-old female presented to our clinic with a 40-year history of persistent hypercalcemia secondary to PHPT. During the time that she was followed up in the endocrine clinic, corrected serum calcium ranged from 2.52 to 2.89 mmol/L [normal value (NV) 2.14-2.58], serum phosphate from 0.76 to 1.32 mmol/L (NV 0.74-1.52) and serum parathyroid hormone (PTH) from 9.73 to 13.9 pmol/L (NV 1.3-7.6). Her menstruation was regular.
She presented with facial deformities caused by multiple mandibular swelling at 8 years old. The investigations did not suggest McCune-Albright syndrome, familial hypocalciuric hypercalcemia or multiple endocrine neoplasia type 1 or 2a. There was no significant family history. She underwent two corrective surgeries for her mandibular deformities. Histopathologic examinations of the excised mandibular tissues confirmed the presence of brown tumors.
Preoperative imaging modalities included neck ultrasonography; angiography to assess the neck vasculature; selective parathyroid venous sampling; radioisotope bone scintiscan (with 12 mCi of technetium-99m methylene diphosphonate) or sestamibi imaging; and sestamibi imaging with single-photon emission computed tomography (SPECT). However, the discordant results of these advanced imaging modalities were not helpful in localizing the parathyroid glands. These issues provided valuable insights into the challenges during her three unsuccessful neck explorations at age 8, 12 and 40.
This patient was lost to follow up in 2000. Ten years later in 2010, she was admitted with acute cholecystitis secondary to cholelithiasis. She had an uneventful cholecystectomy. During admission, she was also assessed for complications of PHPT. Bilateral nephrocalcinosis, corneal calcifications and worsening skeletal manifestations of PHPT were found. The skeletal changes included periosteal bone resorption and acro-osteolysis of the hands (Figure 1). There was no evidence of fractures and renal dysfunction. A subnormal 25-hydroxycholecalciferol [25(OH)D] level of 41.1 nmol/L (NV 60.0-160.0) was also noted. Dual energy x-ray absorptiometry (DEXA) scan of the lumbar vertebrae and left hip demonstrated normal bone mineral density with z-scores of 0.4 and 2.8, respectively.

Figure 1. AP radiograph of the left hand, cropped to accentuate osseous detail. Areas of subperiosteal resorption are seen markedly at the radial aspect of the third middle phalanx, and subtly at the radial aspect of the second middle phalanx (arrows). Acro-osteolysis is also evident at the distal phalanges (arrowheads).
At the time when the patient was diagnosed with PHPT, sodium dihydrogen phosphate was the medical treatment for persistent hypercalcemia. Subsequently, cinacalcet was added when it became available. Unfortunately, she experienced adverse adverse effects from cinacalcet: persistence of poor appetite, nausea and vomiting led discontinuation of the drug for one month. When cinacalcet was reinitiated, the dose was titrated upward gradually to the optimal dosage of 25 mg twice daily without severe adverse gastrointestinal effects. Ergocalciferol (vitamin D2), at a dosage of 0.25 µg daily (titrated based on the calcium level) was also started for her subnormal serum 25(OH)D level.
The patient was closely monitored for recurrent swelling and purulent discharge associated with mandibular osteomyelitis. Her alkaline phosphatase (ALP) levels remained relatively stable (600 to 870 U/L) for the first 24 years (NV 40-150 U/L). The subsequent two-fold to three-fold rise in the ALP (1,600 to 2,000 U/L) correlated with recurrent osteomyelitis in the mandible. Computed tomography (CT) showed thinning and sclerotic changes in the mandible with multiple lucent areas (Figure 2). Cystic lesions with well-circumscribed sclerotic margins were suggestive of brown tumors. However, in view of persistent osteomyelitis, no biopsy was carried out.
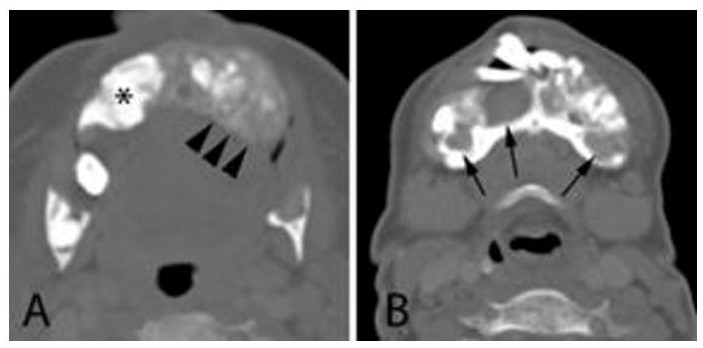
Figure 2. Cross-sectional CT of the mandible in bone algorithm at the level of the mandibular angles (A) and symphysis menti (B). There is a loss of cortical and marrow differentiation. This has been replaced by a ground glass density, with areas of irregular osseous expansion (arrowheads in A) and patchy regions of osteosclerosis (asterisk in A). Cystic lesions with well-circumscribed sclerotic margins (arrows in B) are likely Brown tumours, with evident dental displacement.
Hydrocephalus on CT was an incidental finding while monitoring the chronic mandibular osteomyelitis. Clinically, she was asymptomatic. She had no papilledema, neurological deficit nor any gait abnormality. Subsequent magnetic resonance imaging revealed a communicating hydrocephalus and diffuse calvarial thickening with intracortical tunnelling (Figure 3). This calvarial thickening caused a reduction in the posterior cranial fossa, including the foramen magnum. The resulting compression on the cerebellum and anterior cervico-medullary junction caused cerebellar tonsillar herniation. A ventriculo-peritoneal shunt was inserted with an uneventful post-surgical course.
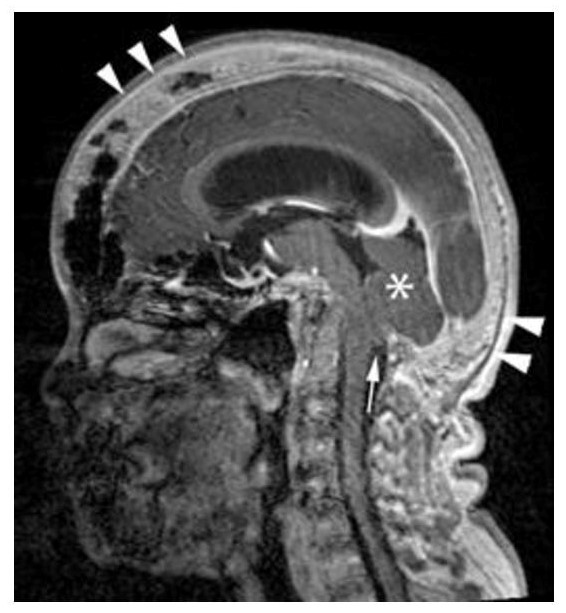
Figure 3. T1 post-gadolinium MRI in midsagittal reconstruction. Calvarial thickening, a known effect of hyperparathyroidism, is apparent (arrowheads). Note the ventricular dilatation and the small posterior fossa (asterisk). Cerebellar tonsillar herniation is depicted (arrow).
The patient exhibited a complex clinical course with multiple disease complications due to elusive abnormal parathyroid glands. The most unusual and significant complication was the complex florid osteitis fibrosis cystica change in the skull. Diffuse calvarial thickening of the skull reduced the posterior cranial fossa and obliterated the foramen magnum, causing local compression on the cerebellum and anterior cervico-medullary junction, leading to cerebellar tonsillar herniation and communicating hydrocephalus. In contrast, the other only case of hydrocephalus was due to the local compression of a brown tumor secondary to PHPT in the maxilla.[3] In addition, the presentation of multiple mandibular brown tumors secondary to asymptomatic PHPT in a child of less than 10 years old has not been reported. Although the previous series of skull brown tumors consisted predominantly of women, they were young and middle-aged adults.[4] In a review of 16 cases involving brown tumors of the skull base, the mean age was 32 years old, and 75% of the patients were women.[5] In another case series of 22 patients with maxillo-facial brown tumors, 91% were women, with a mean age of 51 years old.[6]
The mechanism pertaining to these florid skull changes is not clear. Excess PTH results in an increase in osteoclastic resorption with subsequent fibrous replacement and reactive osteoblastic activity.[7] Osteosclerotic changes are an unusual feature of PHPT, and only 3 cases of multiple skull osteosclerotic lesions in PHPT patients have been reported. One was a 26-year old man with PHPT, while 2 women had coexisting vitamin D deficiency.[7],[8] Diffuse and patchy osteosclerosis has been described in cases of secondary hyperparathyroidism in renal osteodystrophy and vitamin D deficiency.[9],[10] This phenomenon has been postulated to be a disproportionate increase in the osteoblastic response after prolonged osteoclastic activity.[11] Our patient exhibited vitamin D insufficiency. In a previous cross-sectional study, vitamin D deficiency did not suggest any impact on the bone microarchitecture.[12] Therefore, the coexistence of vitamin D insufficiency (41.1 nmol/L) and prolonged PTH exposure could not fully account for the marked skull and skeletal manifestations.
Although the clinical presentation of PHPT has changed over the years due to early detection and treatment, the challenges of localizing and surgically removing elusive parathyroid adenomas have remained, as in our patient.[13] Abnormal parathyroid glands, variable anatomy and ectopic location of adenomas account for most of surgical failures.[14] In cases like ours, localization of the parathyroid gland is essential for preoperative planning.[15] Despite the availability of different advanced imaging modalities for targeted parathyroidectomies, there is still no clear consensus on the preferred imaging strategy.[16] Ultrasonography of the parathyroid glands has sufficient sensitivity (76 to 82%) to detect a single parathyroid enlargement in the neck, but has limited use in multiple gland hyperplasias, double adenomas, the presence of concomitant thyroid nodules and ectopic gland locations.[16] Therefore, ultrasonography alone was not sufficient in our patient given the presence of thyroid nodules, abnormal parathyroid glands, and the possible ectopic or unusual location.
Selective venous sampling has been available since the 1980s. Since our patient initially underwent an unsuccessful parathyroidectomy, angiography of the neck vasculature and selective venous sampling may have been beneficial. Unfortunately, together with the dual phase sestamibi scan and sestamibi scan with SPECT imaging modalities, the location of the parathyroid glands remained undetermined. Unusual anatomical location, multiple glands, and coexistent thyroid nodules may reduce the sensitivities of all these imaging modalities.
Inevitably, in such cases, medical treatment plays an essential role in lowering the serum calcium level and in bone protection.[17] Unfortunately, most pharmaceutical options have only been available in the last decade, with limited long-term outcome data. Sodium dihydrogen phosphate was the first oral therapy available before cinacalcet.[18] However, large and frequent dosing affected compliance, explaining the fluctuation of serum calcium levels in our patient. During the period when the patient was lost to follow up, her calcium control was suboptimal.
Cinacalcet has only been available recently. It appears to stabilize and maintain normocalcemia over time, but has no effects on the bone.[19] Moreover, adverse gastrointestinal effects may affect the optimization of the cinacalcet dose. In addition, a low vitamin D status has been shown to be associated with specific features reflecting more severe biochemical hypercalcemia in postmenopausal women.[12],[20] Supplementing with high dose vitamin D has been shown to be safe in PHPT cases in a randomized controlled trial (RCT), with improvement in vitamin D status and decrease in PTH levels without increasing serum calcium levels.[21] While there have been no RCT evaluating the combination of cinacalcet and vitamin D supplementation, our patient benefited from this combination with an optimal reduction in her serum calcium level without adverse effects.
Severe calvarial osteosclerosis compressing the posterior fossa and causing communicating hydrocephalus due to persistent PHPT is rare. To the best of our knowledge, rare florid diffuse bony changes in the posterior fossa causing brain tissue compression and communicating hydrocephalus have not been previously reported in the literature. An awareness of this rare skull manifestation causing posterior brain compression and communicating hydrocephalus is essential for early diagnosis and prompt intervention to prevent fatal posterior brain herniation.
The available medical options offer both advantages and drawbacks. Moreover, the considerable variation in protracted PHPT presentations necessitates individualized management. Continual active surveillance for unusual complications is essential for early detection and prompt treatment.
Ethical ConsiderationPatient consent was obtained before submission of the manuscript.
Statement of AuthorshipAll authors certified fulfillment of ICMJE authorship criteria.
Author DisclosureThe authors declared no conflict of interest.
Funding SourceNone.
[1] Singh Ospina NM, Rodriguez-Gutierrez R, Maraka S et al. Outcomes of parathyroidectomy in patients with primary hyperparathyroidism: A systematic review and meta-analysis. World J Surg. 2016;40(10):2359-77. PubMed CrossRef