Paget’s Disease of the bone (PDB) is a chronic bone disorder characterized by focal areas of excessive osteoclastic resorption accompanied by a secondary increase in osteoblastic activity, resulting in abnormal bone structure, fractures and deformity.[1] The disease is often asymptomatic and commonly seen in an aging population. PDB typically affects more than one bone in the body with frequently affected bones include the pelvis, vertebrae, skull, femur and tibia.[2],[3] The majority of the patients do not seek medical treatment unless there is associated pain or other related symptoms. Moreover, there are rarely neurologic complications associated with compression of intraspinal nerve tissues.[2] The simultaneous occurrence of PDB of the bone and bony metastases from adenocarcinoma of the lung in the same patient is uncommon.
CASEA 69-year-old female with history of type 2 diabetes, hypertension and dyslipidemia complained of intermittent left hip pain for 3 years with constitutional symptoms. She denied any headache, hearing loss, tinnitus, back pain, joint pain or failure symptoms. There was no history of fracture, trauma or heart failure. On examination, she was unable to ambulate due to her left hip pain. There was no bowing of tibia or femur. Apart from her left hip, her musculoskeletal examinations of other joints and neurological examination were unremarkable. Biochemical tests revealed normal serum calcium and phosphorus with markedly raised alkaline phosphatase (Table 1). The initial differential diagnoses were osteoarthritis, osteoporosis, secondary metastasis or metabolic bone diseases. Her X-ray of the hip revealed diffuse sclerotic left pelvic bone and Magnetic Resonance Imaging (MRI) of the hip revealed extensive marrow signal abnormalities at the left pelvic bone (Figure1). The radiological images above were reported as primary, metastatic bone disease or other metabolic bone disorders like PDB. As part of workup of bony lesion in adult to rule out possibility of secondary malignancy, contrast enhanced computed tomography of thorax, abdomen and pelvis (CECT-TAP) were performed which revealed a spiculated lung nodule at the left lower lung lobe, suggestive of lung malignancy (Figure 2).
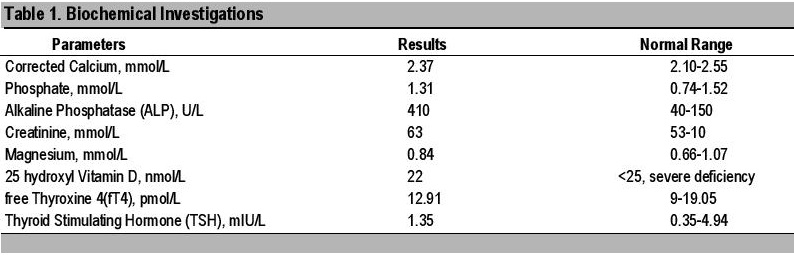
Table 1. Biochemical investigations
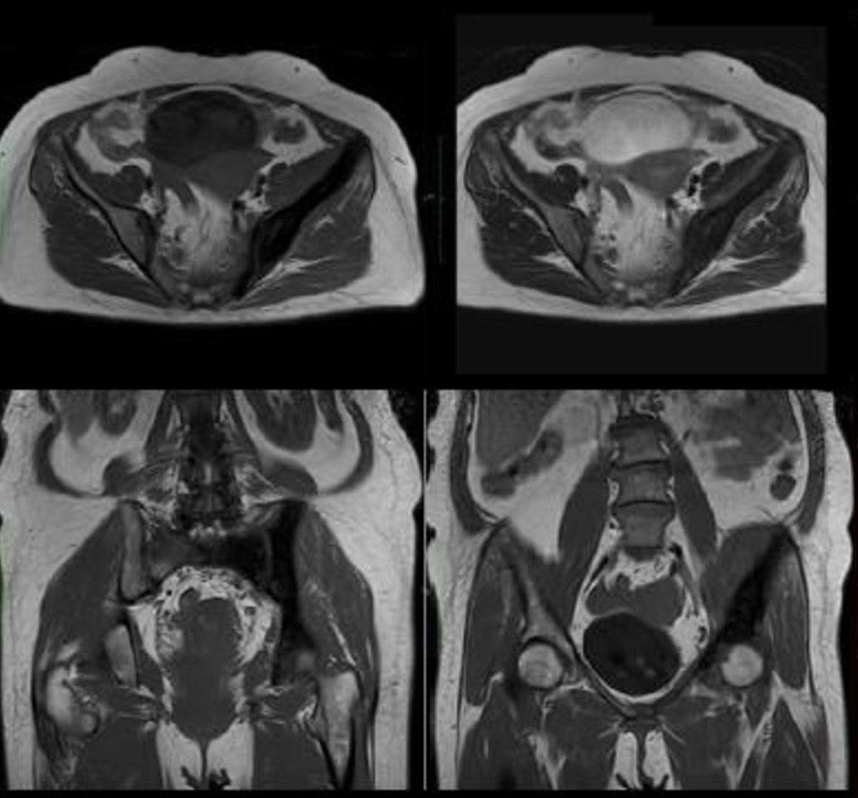
Figure 1. MRI of the hip revealed that there were extensive marrow signal abnormalities of left pubic bone with mild expansion seen in sacrum predominantly left side seen at axial plane (above) and coronal plane (below). The findings were suggestive of primary or metastatic bone disease or other metabolic bone disorder like PDB.
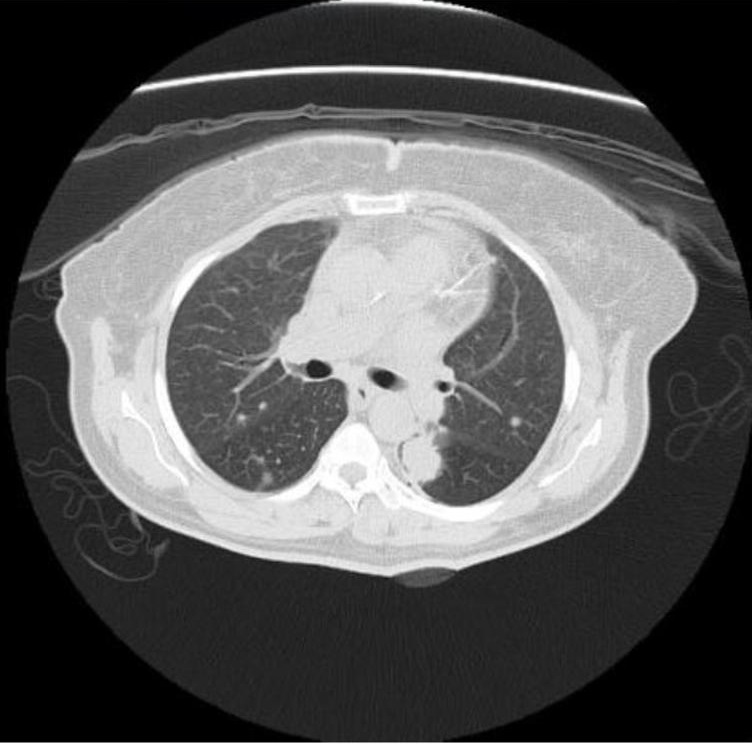
Figure 2. CE CT of thorax revealed that there was a spiculated lung nodule in the superior segment of left lower lobe, adjacent to the left oblique fissure, measuring 2.6 x 1.8 x 2.5 cm (AP x W x CC) associated with thickening of the adjacent left oblique fissure.
In order to ascertain the lesion being a primary, metastatic bone tumour or PDB, an open biopsy of the left iliac bone was done. The histopathology result of bone biopsy of the left iliac bone was later reported as Paget’s disease of the bone (Figure 3). A CT guided biopsy of the lung mass was done later which revealed adenocarcinoma of the lung (Figure 4). She had 18F-FDG PET-CECT Scan for staging evaluation and showed intense tracer uptake in the left lower lobe of the lung with multiple mediastinal lymph nodes as well as right sacral bone, right ilium and bodies of L3-L5 suggestive of new bony metastases. There was also diffuse sclerosis of the left hemi pelvis (ilium, ischium and pubic bone) with minimal metabolic activity in keeping with PDB (Figure 5A and B). The final diagnosis was metastatic bone disease secondary to adenocarcinoma of the lung with underlying PDB. Dual energy X-ray absorptiometry (DEXA) scan was unable to be interpreted due to osteoblastic changes at the lumbar spine and hip. Her echocardiogram did not show any systolic or diastolic dysfunction.
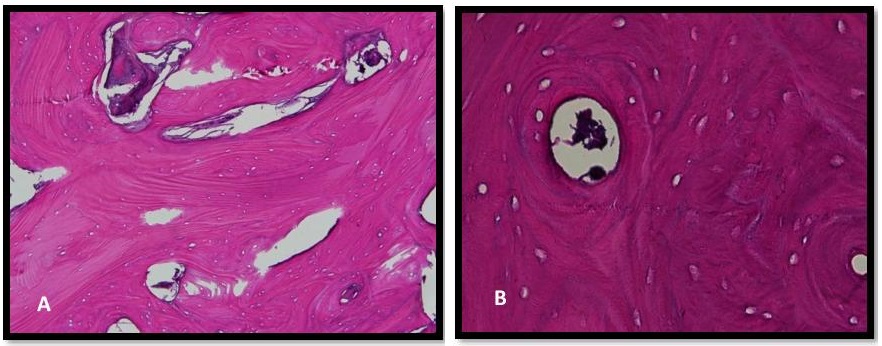
Figure 3. Histopathologic examination of the left iliac bone showed (A) thickening and disorganized trabecular pattern (H & E, 40x). (B) Cement lines along the coarsened and enlarged trabeculae are characteristically seen. The marrow was calcified and replacement of the marrow space by fibrous tissue was seen (H & E, 40x).
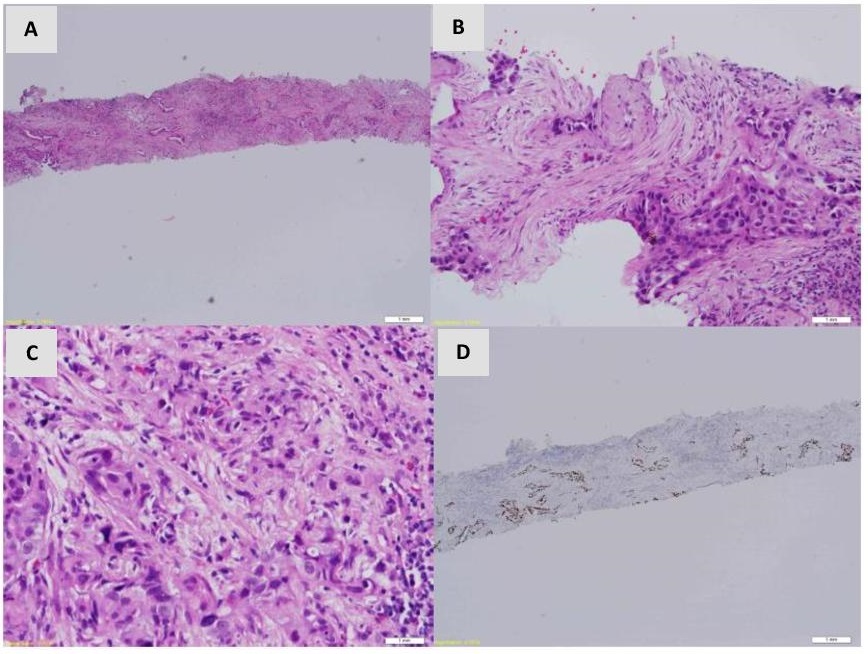
Figure 4. Lung biopsy showed moderately differentiated adenocarcinoma. (A), (B) There were 2 fragments of fibrocollagenous tissue and alveolar tissue displaying infiltration by tumour cells in small cluster, glandular and single cell pattern (H & E, 10x, 20x) (C) The tumour cells exhibit moderate pleomorphism with hyperchromatic nuclei and moderate amount of eosinophilic cytoplasm (H & E, 40x) (D) Immunohistochemistry study shows the tumour cells are positive for transcription factor (TTF-1) (10x).
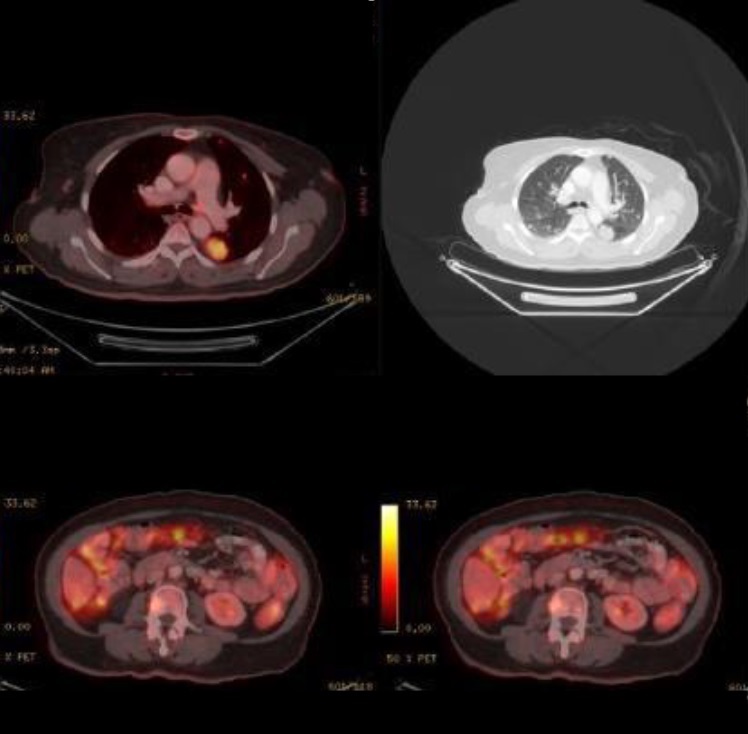
Figure 5A. 18F-FDG PET/CT revealed that there was a hypermetabolic lung mass (SUV max 7.3) measuring 2.7x2.1x3.7cm at left lower lobe of the lung corresponded to the hypodense lesion at CT scan. There was a new hypermetabolic activity in patchy areas of lucency and sclerosis of the right side of sacral bone, right ilium, bodies of L3-L5 and right lamina of L5.
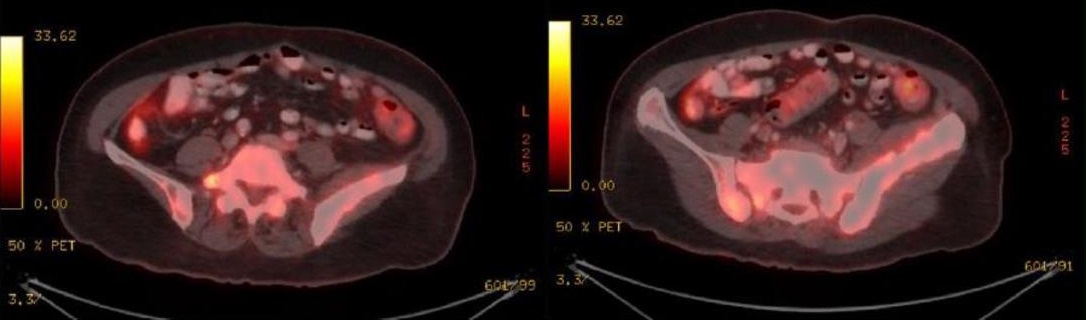
Figure 5B. 18F-FDG PET/CT revealed that there was diffuse sclerosis of the left hemi pelvis (ilium, ischium and pubic bone) with minimal metabolic activity in keeping with PDB.
Figure 5. CE CT of thorax revealed that there was a spiculated lung nodule in the superior segment of left lower lobe, adjacent to the left oblique fissure, measuring 2.6 x 1.8 x 2.5 cm (AP x W x CC) associated with thickening of the adjacent left oblique fissure.
Patient was initiated on high dose Vitamin D and subsequently IV Zoledronic acid for the treatment of the PDB. In view of the stage 4 lung adenocarcinoma with bony metastases, patient was scheduled for palliative systemic chemotherapy.
PDB is a chronic, progressive bone disease of unknown etiology with unevenly increased osteoclastic and osteoblastic skeletal remodelling. It is commonly diagnosed in northern Europe, North America, Australia, and New Zealand, but is rare in the Asia, including Malaysia.[4],[5] About 3.7% of individuals of Anglo-Saxon origin older than the age of 55 are afflicted with PDB.[6],[7],[8],[9] It rarely manifest itself clinically before age 40, and the frequency of the condition increases with advancing age. The disease can be divided into three phases of increasing clinical and radiographic severity: 1) initial resorptive/osteolytic phase, 2) mid-phase, mixed osteoblastic/osteoclastic hyperplasia and 3) late sclerotic phase.[10]
The diagnosis of the disease is based as a whole on clinical presentation, radiological findings and biochemical markers of bone turnover. Since PDB is a chronic progressive disease with minimal symptoms, there is a high possibility that the PDB was pre-existing and there were new bony metastases due to lung adenocarcinoma. Markedly elevated serum alkaline phosphatase (ALP) is a constant feature while calcium and phosphate levels are typically within normal limits. However, about 15% patients present with normal serum ALP level and isoenzymes of ALP.[11] On the other hand, metastatic bony disease can cause disruption of the normal homeostasis of bone which results in skeletal complications such as bone pain, fractures and paraneoplastic syndrome like hypercalcemia.[12] Serum ALP level, as mentioned above, can also be elevated in metastatic bone disease as the degree of ALP elevation is a general measure of metabolic activity. In PDB, the increased ALP not only correlates well with the changes on bone resorption but also the extent of skeletal involvement assessed from either radiographs or scintigraph[13] and the probability of achieving normal values with a potent bisphosphonate.[14] Serum amino-terminal propeptide of type 1 collagen (P1NP) as a measure of bone formation and resorption markers such as serum Beta C-terminal propeptide of type 1 collagen (bCTx) or urine N-terminal propeptide of type 1 collagen (NTx) provide accurate estimates of baseline bone metabolic activity and the response to treatment in patients with PDB.[14] The use of bone turnover markers including the bone formation and resorption markers has been investigated for diagnostic and prognostic purposes in advanced cancer patients.[12]
A single 5-mg dose of IV Zoledronate is the recommended choice of treatment in PDB. In two clinical trials, Zoledronate comparing with risedronate showed Zoledronate provided a more rapid onset of action, and superior effects on quality of life, including pain relief.[15],[16] A follow-up study that compared the duration of remissions with these two treatments showed that Zoledronate produced more frequent, more complete, and more sustained responses to therapy. It allowed normalization of bone turnover markers and improvements in quality of life for many years in most patients after only a single infusion.[16] However, potent bisphosphonates can produce symptomatic hypocalcemia in the presence of marked vitamin D deficiency. In those at risk of vitamin D deficiency, supplementation before treatment is advisable prior to treatment which was applied in our case.[9],[17]
Patients with PDB presenting with bony metastases is rarely reported. Among the previously published cases that reported coexistence of PDB and metastatic bone disease, the primary sites of malignancy were the breast, lung, and prostate.[18],[19],[20],[21] In our patient, the final diagnosis of metastatic bone disease secondary to adenocarcinoma of the lung was found after PDB was diagnosed by bone biopsy. As illustrated in the case, three modalities, including radiography, bone biopsy and 18F-FDG PET/CT were utilized in the diagnostic process. The radiographic and bone biopsy findings and the elevation of the ALP level were compatible with PDB.
Bone biopsy is a minimally invasive procedure performed to evaluate bone abnormalities by sampling and detecting abnormal bone tissue. It is used in diagnosing any of the primary bone malignancy, secondary metastatic bone disease and metabolic bone disorders. The bone biopsy can be performed using fine needle aspiration technique, core biopsy technique or open biopsy technique wherein the region is removed for analysis. In the past, the histology of PDB had focused on iliac crest bone or vertebrae. Hyperosteoclastosis and poor definition of the boundary between cortical and medullary bone are the main histological findings in PDB.[22] Additionally, pagetic bone is also characterized by multinucleated osteoclasts with more than 12 nuclei per cell were frequently found at the trabecular surface. A typical appearance of deep resorption lacunae with the so-called swallowtail pattern also observed in the iliac crest biopsies.[23]
A previous report revealed no statistical correlation between 18F-FDG uptake and the serum ALP level in patients with PDB.24 Majority of patients with PDB revealed no abnormal 18F-FDG uptake that suggested absence of relationship between increased osteoblastic or osteoclastic activity with the increased use of glucose.24 Therefore, there is a potential to utilise different grade of 18F-FDG uptake to discriminate between benign PDB and metastatic bone disase.[24] However, low-grade uptake may be seen in patients with more active disease indicated by higher ALP. Rarely, PDB could be a possible cause of false-positive scans in elderly patients who are being assessed for metastatic disease. Previous case reports of increased tracer uptake in Paget’s disease mimicking metastasis in a case of malignant mesothelioma and rectal cancer have been reported.[25],[26]
This case highlighted the possible coexistence of PDB and bony metastasis in a patient. Both diseases require careful evaluation to permit appropriate therapies to be instituted albeit for both conditions. Therefore, in cases which are of a diagnostic challenge, a bone biopsy may be essential to establish the diagnosis.
Ethical ConsiderationPatient consent was obtained before submission of the manuscript.
Statement of AuthorshipAll authors certified fulfillment of ICMJE authorship criteria.
Author DisclosureAll the authors declared no conflict of interest.
Funding SourceNone.
[1] Selby PL, Davie MW, Ralston SH, et al. Guidelines on the management of Paget's disease of bone. Bone. 2002;31(3):366–73. PubMed