Pulse Oximetry as a Screening Test for Hemodynamically Significant Lower Extremity Peripheral Artery Disease in Adults with Type 2 Diabetes Mellitus*✝︎
Ria Mari Siao,* Marc Josef So,** Maria Honolina Gomez*,***
*Presented at the 2018 Philippine Society of Endocrinology, Diabetes and Metabolism, Inc. (PSEDM) Philippine Research Initiatives on Diabetes and Endocrinology (PRIDE) session held at the EDSA Shangri-La Hotel, Mandaluyong, Philippines on March 22, 2018.
✝︎Presented at the 48th Philippine College of Physicians Annual Convention held at the SMX Convention Center, Pasay, Philippines on April 30, 2018.
Ria Mari Siao, MD
Section of Endocrinology, Diabetes and Metabolism, Department of Medicine
University of Santo Tomas Hospital
España Boulevard, 1015, Manila, Philippines
Tel. No.: +632-7313001 local 2455
E-mail: lilswallow@yahoo.com
ORCID: https://orcid.org/0000-0001-7704-3509
e-ISSN 2308-118x
Printed in the Philippines
Copyright © 2018 by the JAFES
Received April 4, 2018. Accepted May 26, 2018.
Published Online First: November 2, 2018.
Objective. The main objective is to determine if digital pulse oximetry is an acceptable screening tool to detect hemodynamically significant lower extremity peripheral artery disease (PAD) in patients 50 years old and above with type 2 diabetes mellitus (T2DM) seen at the University of Santo Tomas Hospital (USTH).
Methodology. A total of 78 subjects (155 limbs) were included. Using duplex ultrasonography as the reference standard for the presence of hemodynamically significant lower extremity PAD, sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV) were obtained for abnormal percent oxygen saturation (SpO2) gradients and for ankle-brachial index (ABI).
Results. Of the 155 limbs, 38.7% had hemodynamically significant stenosis. Pulse oximetry had 76.7% sensitivity (95% CI, 65.2% to 88.1%), 85.3% specificity (95% CI, 78.0% to 92.6%), 76.7% PPV (95% CI, 66.5% to 84.4%) and 85.3% NPV (95% CI, 78.4% to 90.2%). ABI had 40.7% sensitivity (95% CI, 30.1% to 51.3%), 88.2% specificity (95% CI, 80.0% to 96.3%), 68.6% PPV (95% CI, 53.6% to 80.4%) and 70.1% NPV (95% CI, 65.1% to 74.5%). Combining both produces 88.1% sensitivity (95% CI, 78.5% to 97.8%), 74.2% specificity (95% CI, 65- 83.4%), 68.4 PPV (95% CI, 60.3% to 75.6%) and 90.8% NPV (95% CI, 83.0% to 95.2%).
Conclusion. The results of this study suggest that pulse oximetry has a higher sensitivity than ABI as a screening tool for hemodynamically significant lower extremity PAD in T2DM patients 50 years old and above. Combining these two tests may be done to achieve a higher sensitivity.
Keywords: type 2 diabetes mellitus, peripheral artery disease, oximetryPeripheral arterial disease of the lower extremities is a condition wherein the lumen of the arteries in the extremities becomes progressively obstructed by plaque, resulting in reduced blood flow to the lower limbs. This is frequently atherosclerotic in origin, and is considered a coronary artery disease equivalent.[1],[2],[3] In the Philippine setting, the prevalence of PAD among the general adult population increased from 0.4% in 2003 to 1.2% in 2008.[4] In patients with diabetes, the prevalence of PAD increases with age, from 20% in those over 40 years of age to 29% in those over 50 years.[5]
While early detection and treatment of PAD may prevent disability and death, the diagnosis is potentially missed because majority of patients are asymptomatic, or present with leg symptoms not typical of intermittent claudication.[6],[7],[8],[9] In the Limburg PAD Study, younger age groups and diabetes were more significantly associated with asymptomatic PAD.[10]
When screening for PAD, relying on history alone may underdiagnose those who are asymptomatic. The gold standard for peripheral arterial disease diagnosis is conventional angiography, but non-invasive vascular imaging modalities such as duplex ultrasonography are more frequently performed. In the clinics, the most widely used screening test for PAD is the ankle-brachial index. Throughout the literature, there is a wide variation in specificity and sensitivity reported by different authors. In a critical review of ABI studies, Khan reported more than 90% sensitivity and more than 95% specificity in diagnosing 50% stenosis of the lower extremity arteries.[11] Similarly, Guo reported 91% sensitivity and 86% specificity for hemodynamically significant stenosis.[3] While ABI has been demonstrated to be highly sensitive and specific in diagnosing PAD in patients with significant stenosis, results have been inconsistent in those with less severe stenosis or with calcified vessels.[12]
The American Diabetes Association (ADA) recommends routinely screening all patients with diabetes above age 50 and in all diabetics with risk factors (e.g. smoking, hyperlipidemia, hypertension or duration of diabetes >10 years) for PAD under age 50.[5] The premise and the interpretation of the ABI is relatively simple: the lower the index, the more severe the disease. While generally accepted as a screening test, the ABI also has some limitations. Factors that may impede proper measurement of blood pressure will affect the ABI reading. Calcification of the peripheral arteries — a phenomenon commonly referred to as medial arterial calcification — can make the arteries incompressible, notably in patients who are elderly, or those with diabetes, chronic kidney disease or rheumatic disease. The ABI tends to be elevated due to artefactual elevations in occlusion pressures. This is an important concern because peripheral arterial disease is more prevalent in these patients compared to the general population.[13],[14],[15],[16],[17]
For patients with diabetes, using the ABI as a screening test for PAD in the clinics may yield false negative results. The Strong Heart Study demonstrated a similar association with mortality in those with high and low ABI, with a suggested upper limit of normal not to exceed 1.40.[18] An option for a screening test that will be unaffected by arterial calcifications would be ideal.
Pulse oximetry measures peripheral blood hemoglobin oxygen saturation. Low blood flow in an extremity produces lower oxygen saturation in the blood.[19],[20] The pulse oximeter works by combining spectrophotometry and optical plethysmography, providing continuous, safe, non-invasive and instantaneous measurement of blood oxygenation without need for any special training.[21] There is no user calibration or site preparation required. The sensors are small, lightweight, easy to apply, noninvasive and readily available. [22] Different brands of pulse oximeters may display different values, depending on the internal calibration of the oximeter.[20] The sensor can also be attached to several locations in the body (e.g. ear lobes, fingertips, toes) that are suitable for monitoring peripheral oxygen saturation. Besides SpO2, most pulse oximeters also offer other display features, including pulse rates. This important feature allows real-time assessment of the quality and reliability of the measurement. If the patient’s heart rate taken by the pulse oximeter differs considerably from the actual heart rate, the SpO2 reading may not be appropriate.
Numerous studies have evaluated and compared the accuracy of different pulse oximeters over a wide range of clinical conditions.[23],[24] In general, the accuracy of most non-invasive pulse oximeters is acceptable for a wide range of clinical applications. Most manufacturers report that their instruments are accurate to ±2% in the SpO2 range of 70 to 100%, and ±3% for saturations between 50% and 69%.[25],[26] Clinical and technical conditions that may affect accuracy include low vascular peripheral perfusion during hypotension, hypothermia, or vasoconstriction; venous congestion leading to artifacts due to venous pulsation; motion artifacts; effect of fetal hemoglobin; and interference by electrical energy and stray light.[24],[27]
The use of pulse oximetry as a non-invasive method in the evaluation of peripheral arterial occlusive disease has been sporadic in the last 20 years. Ignjatović reported reduced SpO2 in tissues vascularized by stenotic atherosclerotic arteries.[28] Results of subsequent studies that investigated the potential of pulse oximetry as a screening test for PAD are conflicting. Kwon and Lee tested SpO2 in 49 patients with known lower extremity arterial disease pre- and post-treatment, defining a decrease of more than 5% in saturation at the toe compared to the finger as an abnormal pulse oximetry result. They reported a sensitivity of 87.06% and a specificity of 87.8%. While the sensitivity, specificity, positive and negative predictive values of SpO2 were not statistically significant, there was a significant improvement in SpO2 post treatment.[29] Parameswaran and colleagues targeted patients with asymptomatic diabetes mellitus, using the toe SpO2 cut-off value of a decrease of 2% lower than the finger or on 12-inch elevation of the foot. They found that pulse oximetry of the toes was comparable to ABI in screening for lower extremity arterial disease, with pulse oximetry having a sensitivity of 77% and a specificity of 97%.[19] Using the same criteria in the study by Parameswaran wherein a patient was considered positive for peripheral vascular disease if at least one of the limbs tested positive, Kumar reported a 74.1% sensitivity and 95% specificity for pulse oximetry in patients with asymptomatic diabetes mellitus.[21] In contrast, another study by Ena and colleagues reported that pocket pulse oximeters showed insufficient sensitivity (42.6%) but acceptable specificity (77.2%) as a screening method for detecting peripheral arterial disease in patients with diabetes mellitus.[30]
In the Philippines, there is limited access to duplex ultrasonography, as it is not available in all areas. If a simple tool like digital pulse oximetry will be found to be useful in screening for peripheral artery disease, the complications of peripheral artery obstruction may be addressed at an earlier time. This study aims to determine if digital pulse oximetry is an acceptable screening tool to detect hemodynamically significant lower extremity PAD among adult patients 50 years old and above with T2DM. Specifically, it seeks to evaluate the sensitivity, specificity, PPV and NPV of digital pulse oximetry using a ≥2% toe-finger oxygen saturation gradient on 12-inch leg elevation in comparison to ABI in the assessment of hemodynamically significant lower extremity artery occlusion compared to arterial duplex ultrasonography as the reference standard. These parameters will also be evaluated in hemodynamically significant lower extremity artery stenosis with areas of total occlusion versus those without areas of total occlusion compared to arterial duplex
METHODOLOGYStudy design and sample size
We performed a cross-sectional criterion-referenced study with arterial duplex ultrasonography as the reference standard on patients 50 years old and above with T2DM seen at the USTH from August to December 2017. Non probability sampling was used (Figure 1).
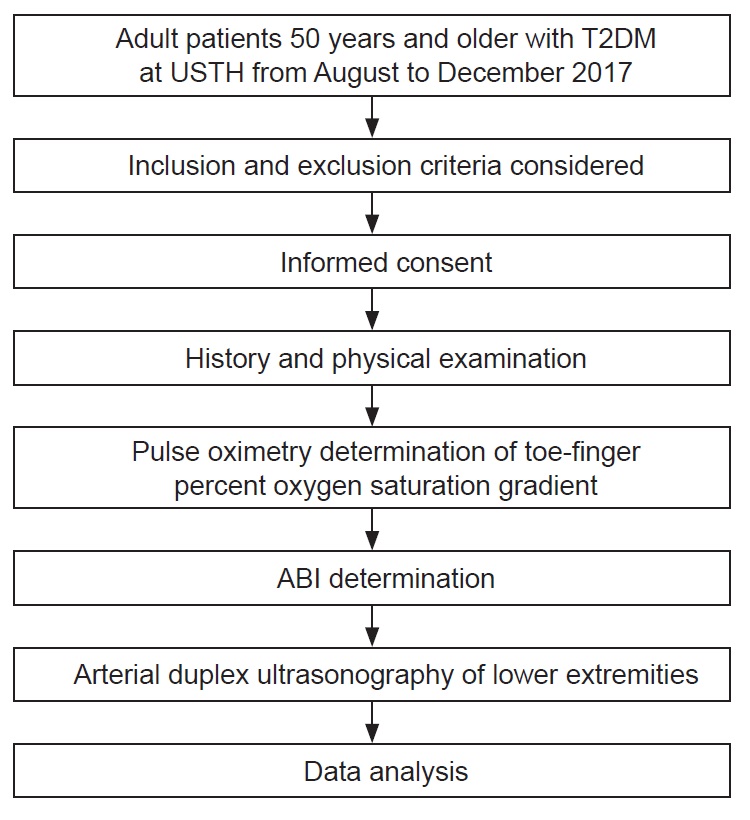
Figure 1. Summary of the study procdures and methods.
With the reported prevalence of PAD in patients with T2DM 50 years old and older to be at 29%, and expected sensitivity of 77% and specificity of 97% for pulse oximetry, given a 95% confidence level and the desired precision of 0.2 for sensitivity, a sample size of 63 patients was needed.[5],[19]
Inclusion and exclusion criteria
Patients 50 years old and above with T2DM seen at the USTH from August to December 2017 were included. Those with comorbidities affecting peripheral limbs (i.e. Raynaud’s, vasculitides) and those on oxygen supplementation were not included in the study. Subjects with nail polish who refused to have it removed were likewise excluded from the study. In patients with amputated limbs, compartment syndrome, or gross skin ulcerations, the involved limb was not included in the study.
Definition of measurement of outcomes
The reference standard for the determination of the presence of lower extremity PAD for this study was its diagnosis via arterial duplex ultrasonography. Participants were placed on a supine position on the examining bed with their lower extremities exposed. The duplex ultrasound scans of the lower limb arteries were performed using the LOGIQ™️ E9 Pro-series by General Electric Japan. The Kappa level (95% confidence interval) of agreement between the duplex ultrasound and angiographic assessments for distinguishing hemodynamically significant (>50%) stenosis was 0.55.[31]
The bilateral lower extremity arterial segments were insonated at an angle of less than 60 degrees, starting at the level of the distal external iliac artery down to the dorsalis pedis artery using a 5-7 MHz linear transducer. For the purpose of this study, only the data from the distal external iliac artery and femoro-popliteal segments were obtained for analysis. In arteries with different categories of lesions, the most severe lesion was taken for comparison. The severity of stenosis was determined by the luminal diameter ratio at the site of the stenosis and the normal adjacent segment, reported as percent diameter reduction. Hemodynamically significant stenosis is defined by a 50 to 99% diameter reduction, including occlusions.[31],[32],[33]
For percent oxygen saturation, a handheld pulse oximeter (HD-76, Wilcare, New Jersey, USA) was applied to the index finger and both great toes with the patient in supine position at room air. If the SpO2 signal was not obtainable due to necrosis or loss, the signal from the next toe was used. The result was positive for PAD if the SpO2 of the big toe taken with the foot in resting position or on 12-inch leg elevation had a difference of at least 2% compared to the index finger SpO2.[19]
ABI measurements were performed using a sphygmomanometer cuff and a handheld Doppler probe (Hadeco® Smart Doppler, Kyoto, Japan). Using the American College of Cardiology Foundation/American Heart Association (ACCF/AHA) and ADA 2003 Consensus Statement definition, an abnormal ankle-brachial index is a value of less than or equal to 0.9.[5],[34]
All pulse oximetry and blood pressure determinations were taken with the patient in supine position at room air. After obtaining consent from the patient, pulse oximetry readings were taken by the primary investigator and recorded in a separate sheet. ABI measurements were performed after pulse oximetry measurements by a separate vascular technician who was blinded to the pulse oximetry readings and clinical profile of the study patients. Arterial duplex ultrasonography was performed by a single trained and experienced vascular technologist blinded to the ABI and pulse volume waveform results. Duplex ultrasonography results were interpreted by a vascular cardiologist blinded to both the pulse oximetry and ABI readings.
Data analysis
Descriptive analysis of baseline characteristics were performed using means and percentages. Using duplex ultrasonography as the reference standard for determination of presence of hemodynamically significant lower extremity PAD, sensitivity, specificity, PPV and NPV were obtained for abnormal SpO2 gradients and for ABI. Since values were obtained at the limb level and not at the patient level, we shall consider the patient as a cluster, and computations were made in consideration for clustered data.[35] Values were obtained using the ratio estimator method for computation for clustered data.[36] Confidence intervals (CI) at 95% were obtained for each value.
Ethical considerations
Pulse oximetry and ABI determination are both non-invasive procedures with no potential harm to the patients. This study was approved by the USTH Institutional Review Board and Ethics Committee. Signed informed consent was obtained from each subject. Privacy and confidentiality of data and results are protected.
Seventy-eight subjects were included in the study, and a total of 155 limbs were evaluated. Half of the subjects were male, with a mean age of 65.6 years and a mean duration of diabetes at 9.6 years. Diabetes medication requirements were varied: 30.8% were on insulin, 50% were on oral medications alone and 19.2% were not on any medications for diabetes at the time of study. Hypertension (74.4%) and dyslipidemia (60.3%) were the most common co-morbidities. Claudication was the most commonly reported symptom (47.4%) (Table 1).
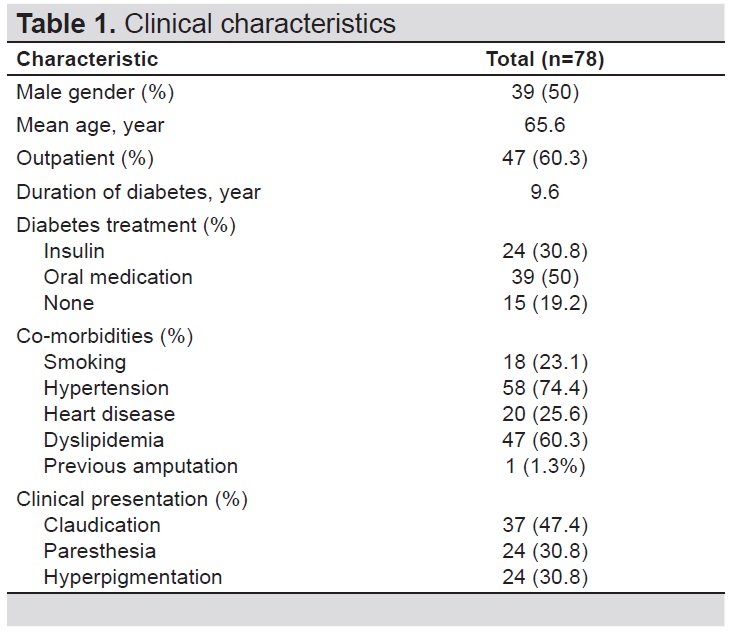
Table 1. Clinical characteristics
Out of 155 limbs, only 9.7% had no evidence of stenosis, with the remaining having mild to severe stenosis with areas of total occlusion (Table 2). Arteries with at least 50% stenosis are deemed hemodynamically significant as these would require treatment.[31] The results showed 38.7% had hemodynamically significant stenosis; of these 60 limbs, 25 had areas of total or 100% occlusion.
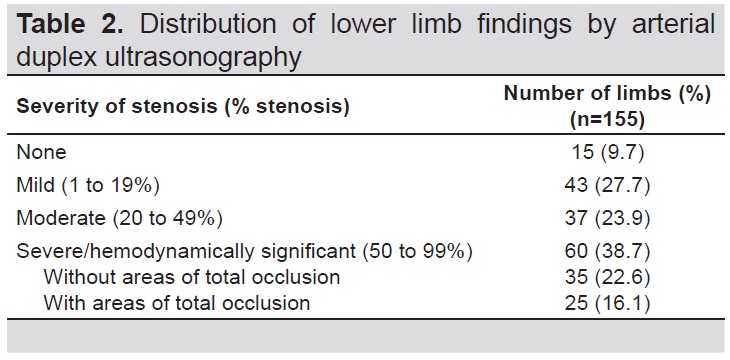
Table 2. Distribution of lower limb findings by arterial duplex ultrasonography
Three of the limbs had open wounds on the foreleg, so that ankle blood pressure and ABI determination were measured in only 152 limbs. An ABI of 0.9 or less was considered as hemodynamically significant peripheral arterial disease equivalent to >50% occlusive stenosis, found in 22.5% of the limbs in the study (Table 3).[5],[37],[38]
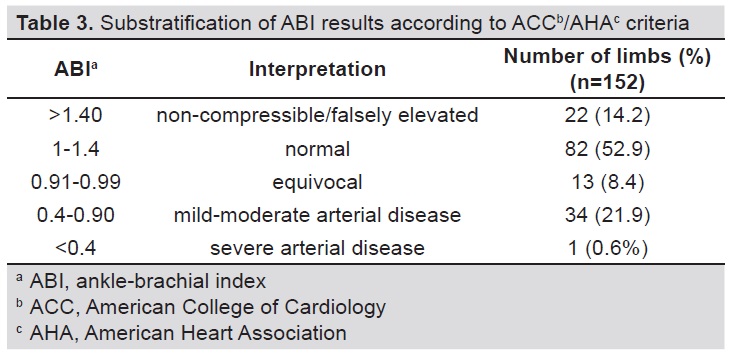
Table 3. Substratification of ABI results according to ACC^b/AHA^c criteria
Of the 155 total limbs included in the study, 60 (38.7%) were positive for peripheral arterial disease using pulse oximetry test criteria (Table 4). Using arterial duplex ultrasonography as the standard, the sensitivity, specificity, PPV and NPV for pulse oximetry were 76.7%, 85.3%, 76.7% and 85.3% respectively. ABI had a lower sensitivity of 40.7% and specificity of 88.2%, yielding a PPV of 68.6% and NPV of 70.1%. Combining pulse oximetry and ABI, with a positive result defined as either a positive pulse oximetry result or an ABI of ≤0.9, sensitivity was determined to be 88.1% and specificity 74.2%, yielding a PPV of 68.4% and NPV of 90.8%.
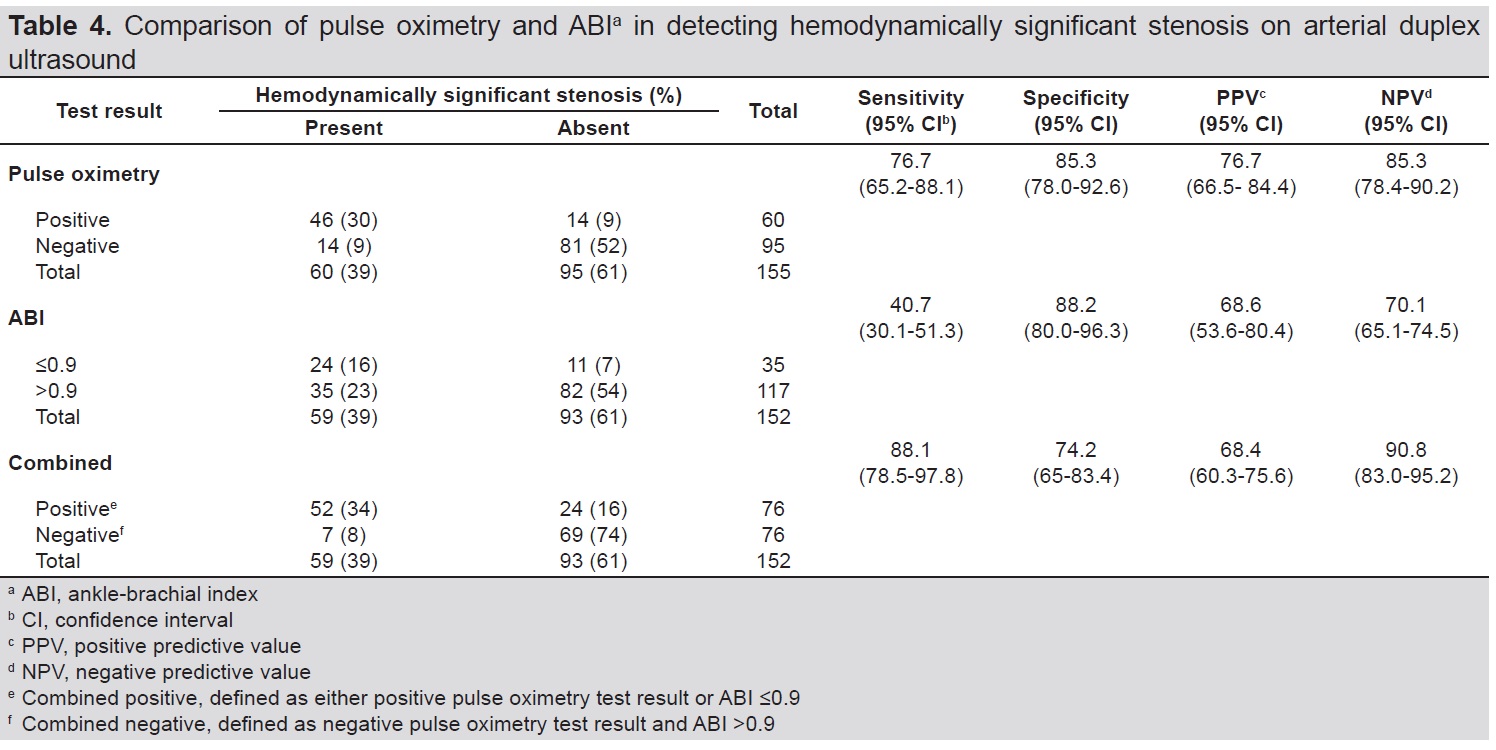
Table 4. Comparison of pulse oximetry and ABI^d in detecting hemodynamically significant stenosis on arterial duplex ultrasound
Duplex ultrasonography can identify arteries with 100% or total occlusion. Findings for limbs with areas of total occlusion are listed in Table 5. Pulse oximetry in these limbs yielded a sensitivity of 92% and a specificity of 71.5%. The PPV and NPV for pulse oximetry were 38.3% and 97.9% respectively. ABI had a 41.7% sensitivity and 80.5% specificity, which gave a 28.6% PPV and 88% NPV. Combining pulse oximetry and ABI yielded a sensitivity of 95.86% and a specificity of 58.6%, which then gave a PPV of 30.3% and a NPV of 98.7%.
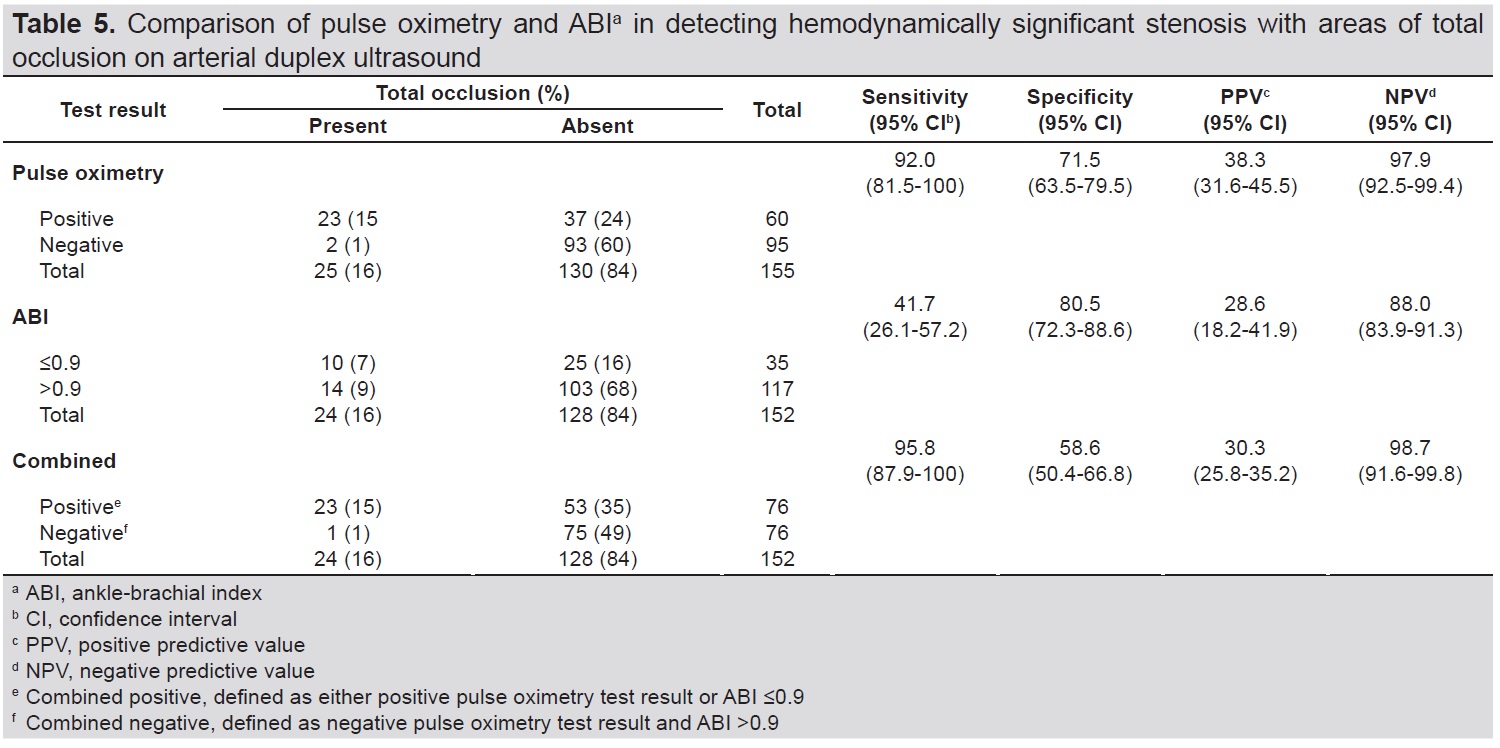
Table 5. Comparison of pulse oximetry and ABI in detecting hemodynamically significant stenosis with areas of total occlusion on arterial duplex ultrasound
In this study population of diabetics of at least 50 years of age, ABI determination was found to have 40.7% sensitivity in detecting hemodynamically significant stenosis. 77% of the subjects had an ABI above the cut-off value of 0.9. However, when further sub-stratified, 14.2% have ABI results of >1.4, attributed to a greater percentage of poorly compressible or falsely elevated ankle pressures. This can be due to medial arterial calcification, which is usually seen in patients with diabetes and in the elderly, underestimating the presence of arterial occlusion. While the ADA recommends performing the ABI as a screening test for patients with diabetes 50 years and above, ABI determination alone is not a sensitive screening test in this particular subset of patients.
Compared to ABI determination, measurement of digital oxygen saturation is not affected by the presence of medial arterial calcification. Abnormal pulse oximetry is defined as a greater than 2% difference between finger and toe oxygen saturation, and can possibly be used to detect lower extremity peripheral arterial disease.[19],[39] However, studies on pulse oximetry and PAD had variable sensitivity results. Studies of the groups of Kwon and Paramesawan included an additional pulse oximetry determination following elevation of the leg from a baseline supine position. This maneuver may account for increased sensitivity in their studies.[19],[29] In our study, we considered the result positive for PAD if the SpO2 of the big toe taken with the foot in resting position or on 12-inch leg elevation had a difference of at least 2% compared to the index finger SpO2. The results showed that pulse oximetry has a sensitivity of 76.7% for the detection of hemodynamically significant stenosis, higher than the sensitivity for ABI.
An ideal screening test is highly sensitive, inexpensive, easy to perform, non-invasive or causes minimal discomfort, and consistent. Both pulse oximetry and ABI determination are inexpensive and non-invasive. In terms of ease and comfort, the investigators have found pulse oximetry to be faster, less complicated to perform and less prone to intra- and inter-observer variability than ABI. Both tests have their respective limitations. In patients with gangrenous digits or extensive wounds, pulse oximetry cannot be performed. In patients with cellulitis, fractures or open wounds in the foreleg, ankle BP determination, likewise, cannot be done. Our results showed that if both pulse oximetry and ABI determination were performed in combination, where either one of the tests being positive would be considered positive for hemodynamically significant stenosis, this produced a higher sensitivity of 88.1% compared to performing either test alone.
PAD prevalence and incidence are known to be both sharply age-related.[40] In our study, 91.3% are at least 50 years old, which may explain the high percentage of lower extremity stenosis on arterial duplex ultrasound, ranging from mild to severe. Out of the 38.7% of limbs with hemodynamically significant stenosis, 41.7% of these limbs had areas of total arterial occlusion. Because of the importance of diagnosing totally occluded arteries, we also tested the sensitivity of pulse oximetry and ABI in detecting limbs with areas of total occlusion (Table 5). Both pulse oximetry and ABI had greater sensitivity in identifying limbs with areas of total occlusion than those with hemodynamically significant stenosis alone. Combining ABI and pulse oximetry yielded a sensitivity of 95.86%. Our findings indicate that pulse oximetry is a sensitive screening tool in detecting limbs with areas of total occlusion.
Strengths and limitations of the study
Our study was able to include a larger number of patients compared to other previous investigations. Having each procedure done by separate individuals minimized measurement bias. A limitation of this study is that it was performed in a single institution.
Recommendations
In order to make this more reflective of the general Philippine population, a multi-center study can be performed with more participants. We recommend more research be done with pulse oximetry and its potential applications. Other areas for research include pulse oximetry pre- and post-exercise, to determine effects on sensitivity in screening for PAD. Correlation of the location of stenosis in the lower extremity with ABI and pulse oximetry test results is another subject of investigation.
In screening for hemodynamically significant lower extremity arterial stenosis in patients with diabetes age 50 years old and above, pulse oximetry had a sensitivity of 76.7%, while ABI determination had a sensitivity of 40.7%. The combination of the two tests increased sensitivity to 88.1%. Screening for lower limb arteries with areas of total occlusion produces higher sensitivity values: 92% for the pulse oximetry, 41.7% for ABI and 95.86% when both tests are combined.
The results of this study suggest that pulse oximetry has a higher sensitivity than ABI as a screening tool for hemodynamically significant lower extremity arterial disease in diabetic patients 50 years old and above. Combining these two tests may be done to achieve a higher sensitivity.
AcknowledgmentsThe authors would like to thank Dr. Phillipp Po and Dr. Elaine Cunanan for their statistical advice.
Statement of AuthorshipAll authors certified fulfillment of ICMJE authorship criteria.
Author DisclosureDr. Siao and Dr. So declared no conflict of interest.
Dr. Maria Honolina S. Gomez has participated in local advisory boards for Boehringer Ingelheim, Novo Nordisk and Pfizer. She also received honoraria as a clinical trial investigator for Takeda, Sanofi Aventis and GlaxoSmithKline. She has received speaker honoraria from Boehringer Ingelheim, Pfizer, Novartis, Novo Nordisk and Torrent Pharmaceuticals. She reports no conflict of interest with regard to this paper.
Funding SourceThis study is a recipient of a financial grant from the Philippine Society of Endocrinology, Diabetes and Metabolism.
[1] Silva Junior JA, Souza DUF, Ferreira DR, et al. Tissue oxygen saturation assessment during claudication symptoms in patients with peripheral arterial disease. J Vasc Bras. 2015;14(4):311-8. CrossRef
[2] Sen S, Lynch DR Jr, Kaltsas E, et al. Association of asymptomatic peripheral arterial disease with vascular events in patients with stroke or transient ischemic attack. Stroke. 2009;40(11):3472-7. PubMed CrossRef
[3] Guo X, Li J, Pang W, et al. Sensitivity and specificity of ankle-brachial index for detecting angiographic stenosis of peripheral arteries. Circ J. 2008;72:605-10. PubMed
[4] Sy RG, Morales DD, Dans AL, et al. Prevalence of atherosclerosis-related risk factors and diseases in the Philippines. J Epidemiol. 2012;22(5):440-7. PubMed PubMed Central
[5] American Diabetes Association. Peripheral arterial disease in people with diabetes. Diabetes Care. 2003;26(12):3333-41. PubMed
[6] Bendermacher BL, Teijink JA, Willigendael EM, et al. A clinical prediction model for the presence of peripheral arterial disease – the benefit of screening individuals before initiation of measurement of the ankle-brachial index: An observational study. Vasc Med. 2007;12(1):5-11. PubMed CrossRef
[7] Mourad JJ, Cacoub P, Collet JP, et al. Screening of unrecognized peripheral arterial disease (PAD) using ankle-brachial index in high cardiovascular risk patients free from symptomatic PAD. J Vasc Surg. 2009;50(3):572-80. PubMed CrossRef
[8] Kallio M, Forsblom C, Groop PH, Groop L, Lepäntalo M. Development of new peripheral arterial occlusive disease in patients with type 2 diabetes during a mean follow-up of 11 years. Diabetes Care. 2003;26(4):1241-5. PubMed
[9] McDermott MM, Guralnik JM, Ferrucci L, et al. Asymptomatic peripheral arterial disease is associated with more adverse lower extremity characteristics than intermittent claudication. Circulation. 2008;117(19):2484-91. PubMed PubMed Central CrossRef
[10] Hooi JD, Stoffers HE, Kester AD, et al. Risk factors and cardiovascular diseases associated with asymptomatic peripheral arterial occlusive disease. The Limburg PAOD Study. Peripheral arterial occlusive disease. Scand J Prim Health Care. 1998;16(3):177-82. PubMed
[11] Khan TH, Farooqui FA, Niazi K. Critical review of the ankle brachial index. Curr Cardiol Rev. 2008;4(2):101-6. PubMed PubMed Central CrossRef
[12] Stein R, Hriljac I, Halperin JL, Gustavson SM, Teodorescu V, Olin JW. Limitation of the resting ankle-brachial index in symptomatic patients with peripheral arterial disease. Vasc Med. 2006;11(1):29-33. PubMed CrossRef
[13] Al-Qaisi M, Nott DM, King DH, Kaddoura S. Ankle brachial pressure index (ABPI): An update for practitioners. Vasc Health Risk Manag. 2009;5:833-41. PubMed PubMed Central
[14] 14. Khammash MR, Obeidat KA, El-Qarqas EA. Screening of hospitalised diabetic patients for lower limb ischaemia: is it necessary? Singapore Med J. 2008;49(2):110-3. PubMed
[15] Jörneskog G. Why critical limb ischemia criteria are not applicable to diabetic foot and what the consequences are. Scand J Surg. 2012;101(2):114-8. PubMed CrossRef
[16] 16. Williams DT, Pugh ND, Coleman DP, Harding KG, Price P. Review: The laboratory evaluation of lower limb perfusion in diabetes mellitus. A clinical review. Br J Diabetes Vasc Dis. 2005;5:64-70. CrossRef
[17] Andersen CA. Noninvasive assessment of lower extremity hemodynamics in individuals with diabetes Mellitus. J Vasc Surg. 2010;52(3 Suppl):76S-80S. PubMed CrossRef
[18] Resnick H, Lindsay RS, McDermott MM, et al. Relationship of high and low ankle brachial index to all-cause and cardiovascular disease mortality: the Strong Heart Study. Circulation. 2004;109(6):733-9. PubMed CrossRef
[19] Parameswaran GI, Brand K, Dolan J. Pulse oximetry as a potential screening tool for lower extremity arterial disease in asymptomatic patients with diabetes mellitus. Arch Intern Med. 2005;165(4):442-6. PubMed CrossRef
[21] Kumar MS, Lohiya A, Ramesh V, Behera P, Palepu S, Rizwan SA. Sensitivity and specificity of pulse oximetry and ankle-brachial index for screening asymptomatic peripheral vascular diseases in type 2 diabetes mellitus. J Assoc Physicians India. 2016;64(8):38-43. PubMed
[22] Mendelson, Y. Invasive and noninvasive blood gas monitoring. In: DL Wise, ed. Bioinstrumentation and biosensors, 1st ed. New York: Marcel Dekker, Inc., 1991.
[23] Merrick EB, Hayes TJ. Continuous, non-invasive measurements of arterial blood oxygen levels. Hewlett-Packard Journal. 1976;28(2):2-9. http://www.hpl.hp.com/hpjournal/pdfs/IssuePDFs/1976-10.pdf
[24] Mendelson Y. Pulse oximetry: theories and applications for non-invasive monitoring. Clin Chem. 1992;38(9):1601-7. PubMed
[25] Razi E, Akbari H. A comparison of arterial oxygen saturation measured both by pulse oximeter and arterial blood gas analyzer in hypoxemic and non-hypoxemic pulmonary diseases. TRJ. 2006;7(2):43-7. https://pdfs.semanticscholar.org/088a/bb5bc4daccc7a5818e96cdea145a011c8fe2.pdf
[26] Jensen LA, Onyskiw JE, Prasad NG. Meta-analysis of arterial oxygen saturation monitoring by pulse oximetry in adults. Heart Lung.1998;27(6):387-408. PubMed
[27] Tungjitkusolmun S. Accuracy versus perfusion. In: JG Webster, ed. Design of pulse oximeters. New York: Taylor & Francis Group, 1997.
[28] Ignjatović N, Vasiljević M, Milić D, et al. Diagnostic importance of pulse oximetry in the determination of the stage of chronic arterial insufficiency of lower extremities. Srp Arh Celok Lek. 2010;138(5-6):300-4. PubMed CrossRef
[29] Kwon JN, Lee WB. Utility of digital pulse oximetry in the screening of lower extremity arterial disease. J Korean Surg Soc. 2012;82(2):94-100. PubMed PubMed Central CrossRef
[30] Ena J, Argente CR, González-Sánchez V, Algado N, Verdú G, Lozano T. Use of pocket pulse oximeters for detecting peripheral arterial disease in patients with diabetes mellitus. JDM. 2013;3(2):79-85. Article ID 31380. CrossRef
[31] Arellano RS, Abola MTB. Diagnosis of arterial disease of the lower extremities with duplex scanning: A validation study. Phil Heart Center J. 2007; 13(2):96-100. https://www.phc.gov.ph/about-phc/journals/pdf/arellano.pdf
[32] Eiberg JP, Grønvall Rasmussen JB, Hansen MA, Schroeder TV. Duplex ultrasound scanning of peripheral arterial disease of the lower limb. Eur J Vasc Endovasc Surg. 2010;40(4):507-12. PubMed CrossRef
[33] Hingorani A, Ascher E, Markevich N, et al. A comparison of magnetic resonance angiography, contrast arteriography, and duplex arteriography for patients undergoing lower extremity revascularization. Ann Vasc Surg. 2004; 18(3):294-301. PubMed CrossRef
[34] 2011 Writing Group Members; 2005 Writing Committee Members, ACCF/AHA Task Force Members. 2011 ACCF/AHA focused update of the guideline for the management of patients with peripheral artery disease (Updating the 2005 Guideline): A report of the American College of Cardiology Foundation/American Heart Association Task Force on practice guidelines. Circulation. 2011;124(18):2020-45. PubMed CrossRef
[35] McCarthy WF, Guo N. The estimation of sensitivity and specificity of clustered binary data. Paper 206-31. SAS Institute Inc. Proceedings of the 31st Annual SAS® Users Group International Conference. Cary, NC: SAS Institute Inc. 2006. http://www2.sas.com/proceedings/sugi31/206-31.pdf
[36] Genç Y, Gökmen D, Tüccar E, Yaǧmurlu B. Estimation of sensitivity and specificity for clustered data. Turk J Med Sci. 2005;35:21-4. http://journals.tubitak.gov.tr/medical/issues/sag-05-35-1/sag-35-1-4-0407-5.pdf
[37] Pollak AW, Norton PT, Kramer CM. Multimodality imaging of lower extremity peripheral arterial disease: Current role and future directions. Circ Cardiovasc Imaging. 2012;5(6):797-807. PubMed PubMed Central CrossRef
[38] Gerhard-Herman MD, Gornick HL, Barrett C, et al. 2016 AHA/ACC guideline on the management of patients with lower extremity peripheral artery disease: Executive summary: A report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. J Am Coll Cardiol. 2017;69(11):1465-1508. PubMed CrossRef
[39] Creager MA, Loscalzo J. Arterial diseases of the extremities. In: DL Kasper, AS Fauci, SL Hauser, eds. Harrison's Principles of Internal Medicine, 19th ed. New York: McGraw Hill Education, 2015.
[40] 40. Criqui MH, Aboyans V. Epidemiology of peripheral artery disease. Circ Res. 2015;116(9):1509-26. PubMed CrossRef
Authors are required to accomplish, sign and submit scanned copies of the JAFES Author Form consisting of: (1) Authorship Certification, that all the requirements for authorship have been met by each author, and that the final version of the manuscript has been read and approved by all authors; (2) the Author Declaration, that the article represents original material that is not being considered for publication or has not been published or accepted for publication elsewhere; (3) the Statement of Copyright Transfer [accepted manuscripts become the permanent property of the JAFES and are licensed with an Attribution-Share Alike-Non-Commercial Creative Commons License. Articles may be shared and adapted for non-commercial purposes as long as they are properly cited]; and the ICMJE form for Disclosure of Potential Conflicts of Interest. For original articles, authors are required to submit a scanned copy of the Ethics Review Approval of their research as well as registration in trial registries as appropriate. For manuscripts reporting data from studies involving animals, authors are required to submit a scanned copy of the Institutional Animal Care and Use Committee approval. For Case Reports or Series, and Images in Endocrinology, consent forms, are required for the publication of information about patients; otherwise, appropriate ethical clearance has been obtained from the institutional review board. Articles and any other material published in the JAFES represent the work of the author(s) and should not be construed to reflect the opinions of the Editors or the Publisher.